

SUCCOR Risk: Design and Validation of a Recurrence Prediction Index for Early-Stage Cervical Cancer
- PMID: 35430668
- PMCID: PMC9246807
- DOI: 10.1245/s10434-022-11671-5
SUCCOR Risk: Design and Validation of a Recurrence Prediction Index for Early-Stage Cervical Cancer
Abstract
Objective: Based on the SUCCOR study database, our primary objective was to identify the independent clinical pathological variables associated with the risk of relapse in patients with stage IB1 cervical cancer who underwent a radical hysterectomy. Our secondary goal was to design and validate a risk predictive index (RPI) for classifying patients depending on the risk of recurrence.
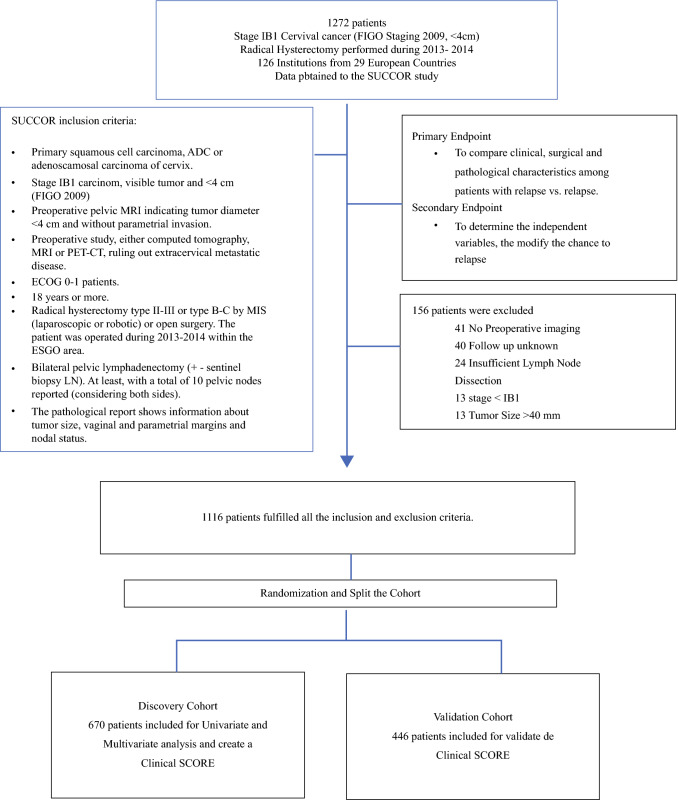
Methods: Overall, 1116 women were included from January 2013 to December 2014. We randomly divided our sample into two cohorts: discovery and validation cohorts. The test group was used to identify the independent variables associated with relapse, and with these variables, we designed our RPI. The index was applied to calculate a relapse risk score for each participant in the validation group.
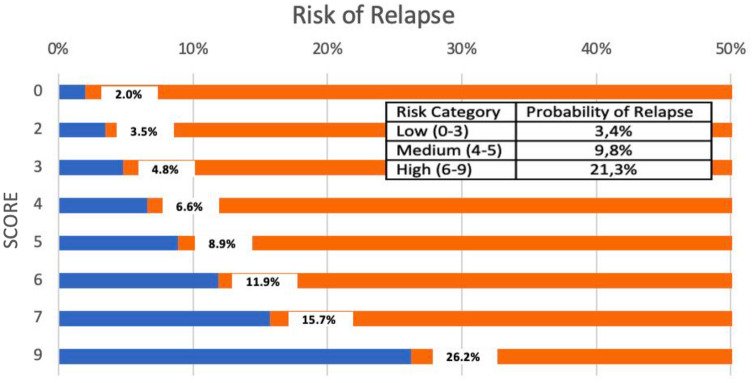
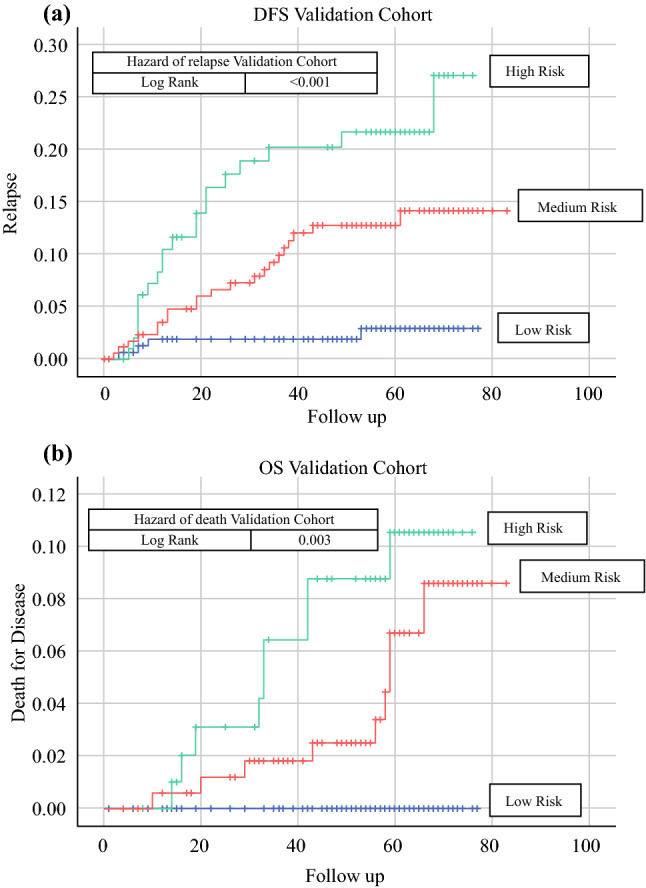
Results: A previous cone biopsy was the most significant independent variable that lowered the rate of relapse (odds ratio [OR] 0.31, 95% confidence interval [CI] 0.17-0.60). Additionally, patients with a tumor diameter >2 cm on preoperative imaging assessment (OR 2.15, 95% CI 1.33-3.5) and operated by the minimally invasive approach (OR 1.61, 95% CI 1.00-2.57) were more likely to have a recurrence. Based on these findings, patients in the validation cohort were classified according to the RPI of low, medium, or high risk of relapse, with rates of 3.4%, 9.8%, and 21.3% observed in each group, respectively. With a median follow-up of 58 months, the 5-year disease-free survival rates were 97.2% for the low-risk group, 88.0% for the medium-risk group, and 80.5% for the high-risk group (p < 0.001).
Conclusion: Previous conization to radical hysterectomy was the most powerful protective variable of relapse. Our risk predictor index was validated to identify patients at risk of recurrence.
© 2022. The Author(s).
Conflict of interest statement
Nabil Manzour, Enrique Chacón, Nerea Martin-Calvo, Felix Boria, José A. Minguez, Juan L. Alcazar, and Luis Chiva have declared no conflicts of interest.
Figures
References
-
- Cibula D, Pötter R, Planchamp F, et al. The European Society of Gynaecological Oncology/European Society for Radiotherapy and Oncology/European Society of Pathology guidelines for the management of patients with cervical cancer. Radiother Oncol. 2018;127(3):404–416. doi: 10.1016/j.radonc.2018.03.003. - DOI - PubMed
