

Impaired coagulation, liver dysfunction and COVID-19: Discovering an intriguing relationship
- PMID: 35431501
- PMCID: PMC8985482
- DOI: 10.3748/wjg.v28.i11.1102
Impaired coagulation, liver dysfunction and COVID-19: Discovering an intriguing relationship
Abstract
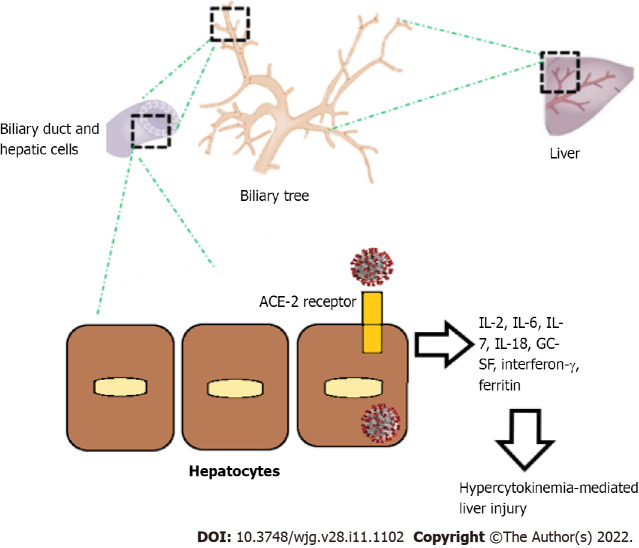
Coronavirus disease 2019 (COVID-19) is, at present, one of the most relevant global health problems. In the literature hepatic alterations have been described in COVID-19 patients, and they are mainly represented by worsening of underlying chronic liver disease leading to hepatic decompensation and liver failure with higher mortality. Several potential mechanisms used by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) to cause liver damage have been hypothesized. COVID-19 primary liver injury is less common than secondary liver injury. Most of the available data demonstrate how liver damage in SARS-CoV-2 infection is likely due to systemic inflammation, and it is less likely mediated by a cytopathic effect directed on liver cells. Moreover, liver alterations could be caused by hypoxic injury and drugs (antibiotics and non-steroidal anti-inflammatory drugs, remdesivir, tocilizumab, tofacitinib and dexamethasone). SARS-CoV-2 infection can induce multiple vascular district atherothrombosis by affecting simultaneously cerebral, coronary and peripheral vascular beds. Data in the literature highlight how the virus triggers an exaggerated immune response, which added to the cytopathic effect of the virus can induce endothelial damage and a prothrombotic dysregulation of hemostasis. This leads to a higher incidence of symptomatic and confirmed venous thrombosis and of pulmonary embolisms, especially in central, lobar or segmental pulmonary arteries, in COVID-19. There are currently fewer data for arterial thrombosis, while myocardial injury was identified in 7%-17% of patients hospitalized with SARS-CoV-2 infection and 22%-31% in the intensive care unit setting. Available data also revealed a higher occurrence of stroke and more serious forms of peripheral arterial disease in COVID-19 patients. Hemostasis dysregulation is observed during the COVID-19 course. Lower platelet count, mildly increased prothrombin time and increased D-dimer are typical laboratory features of patients with severe SARS-CoV-2 infection, described as "COVID-19 associated coagulopathy." These alterations are correlated to poor outcomes. Moreover, patients with severe SARS-CoV-2 infection are characterized by high levels of von Willebrand factor with subsequent ADAMTS13 deficiency and impaired fibrinolysis. Platelet hyperreactivity, hypercoagulability and hypofibrinolysis during SARS-CoV-2 infection induce a pathological state named as "immuno-thromboinflammation." Finally, liver dysfunction and coagulopathy are often observed at the same time in patients with COVID-19. The hypothesis that liver dysfunction could be mediated by microvascular thrombosis has been supported by post-mortem findings and extensive vascular portal and sinusoidal thrombosis observation. Other evidence has shown a correlation between coagulation and liver damage in COVID-19, underlined by the transaminase association with coagulopathy, identified through laboratory markers such as prothrombin time, international normalized ratio, fibrinogen, D-dimer, fibrin/fibrinogen degradation products and platelet count. Other possible mechanisms like immunogenesis of COVID-19 damage or massive pericyte activation with consequent vessel wall fibrosis have been suggested.
Keywords: COVID-19; Coagulation; Liver; SARS-CoV-2.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: There is no conflict of interest associated with the authors of this manuscript.
Figures
References
-
- D'Ardes D, Pontolillo M, Esposito L, Masciarelli M, Boccatonda A, Rossi I, Bucci M, Guagnano MT, Ucciferri C, Santilli F, Di Nicola M, Falasca K, Vecchiet J, Schael T, Cipollone F. Duration of COVID-19: Data from an Italian Cohort and Potential Role for Steroids. Microorganisms. 2020;8 - PMC - PubMed
-
- Gupta A, Madhavan MV, Sehgal K, Nair N, Mahajan S, Sehrawat TS, Bikdeli B, Ahluwalia N, Ausiello JC, Wan EY, Freedberg DE, Kirtane AJ, Parikh SA, Maurer MS, Nordvig AS, Accili D, Bathon JM, Mohan S, Bauer KA, Leon MB, Krumholz HM, Uriel N, Mehra MR, Elkind MSV, Stone GW, Schwartz A, Ho DD, Bilezikian JP, Landry DW. Extrapulmonary manifestations of COVID-19. Nat Med. 2020;26:1017–1032. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
