

Cooling to Hypothermic Circulatory Arrest by Immersion vs. Cardiopulmonary Bypass (CPB): Worse Outcome After Rewarming in Immersion Cooled Pigs
- PMID: 35431978
- PMCID: PMC9008231
- DOI: 10.3389/fphys.2022.862729
Cooling to Hypothermic Circulatory Arrest by Immersion vs. Cardiopulmonary Bypass (CPB): Worse Outcome After Rewarming in Immersion Cooled Pigs
Abstract
Introduction: Cooling by cardiopulmonary bypass (CPB) to deep hypothermic cardiac arrest (HCA) for cardiac surgical interventions, followed by CPB-rewarming is performed on a routine basis with relatively low mortality. In contrast, victims of deep accidental hypothermia rewarmed with CPB generally have a much worse prognosis. Thus, we have developed an intact pig model to compare effects on perfusion pressures and global oxygen delivery (DO2) during immersion cooling versus cooling by CPB. Further, we compared the effects of CPB-rewarming between groups, to restitute cardiovascular function, brain blood flow, and brain metabolism.
Materials and methods: Total sixteen healthy, anesthetized juvenile (2-3 months) castrated male pigs were randomized in a prospective, open placebo-controlled experimental study to immersion cooling (IMM c , n = 8), or cooling by CPB (CPB c , n = 8). After 75 minutes of deep HCA in both groups, pigs were rewarmed by CPB. After weaning from CPB surviving animals were observed for 2 h before euthanasia.
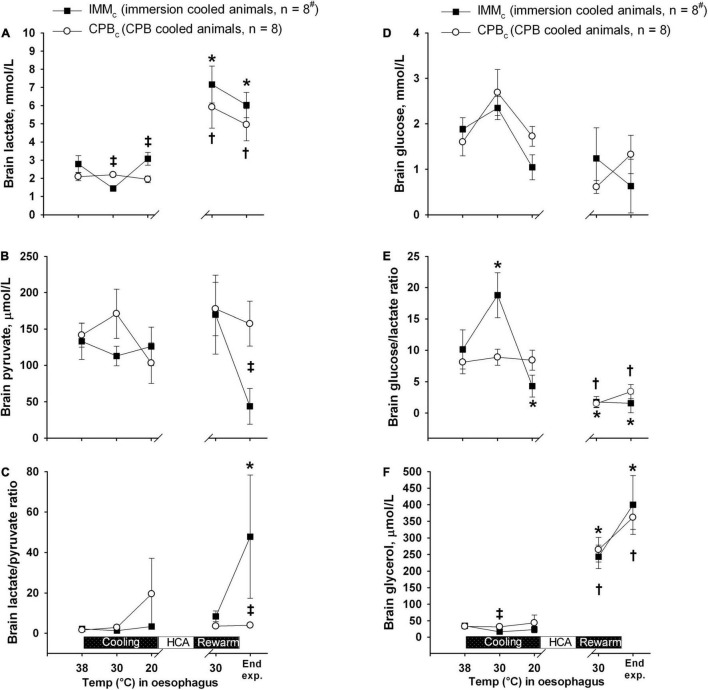
Results: Survival rates at 2 h after completed rewarming were 4 out of 8 in the IMM c group, and 8 out of 8 in the CPB c group. Compared with the CPB c -group, IMM c animals showed significant reduction in DO2, mean arterial pressure (MAP), cerebral perfusion pressure, and blood flow during cooling below 25°C as well as after weaning from CPB after rewarming. After rewarming, brain blood flow returned to control in CPB c animals only, and brain micro dialysate-data showed a significantly increase in the lactate/pyruvate ratio in IMM c vs. CPB c animals.
Conclusion: Our data indicate that, although global O2 consumption was independent of DO2, regional ischemic damage may have taken place during cooling in the brain of IMM c animals below 25°C. The need for prolonged extracorporeal membrane oxygenation (ECMO) should be considered in all victims of accidental hypothermic arrest that cannot be weaned from CPB immediately after rewarming.
Keywords: cardiac index; cardiopulmonary bypass; hypothermia accidental; hypothermia induced; immersion cooling; rewarming.
Copyright © 2022 Filseth, Hermansen, Kondratiev, Sieck and Tveita.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures







References
-
- Baumgartner W. A., Silverberg G. D., Ream A. K., Jamieson S. W., Tarabek J., Reitz B. A. (1983). Reappraisal of cardiopulmonary bypass with deep hypothermia and circulatory arrest for complex neurosurgical operations. Surgery 94 242–249. - PubMed
LinkOut - more resources
Full Text Sources