

Efficacy of Disease Modifying Therapies in Progressive MS and How Immune Senescence May Explain Their Failure
- PMID: 35432156
- PMCID: PMC9009145
- DOI: 10.3389/fneur.2022.854390
Efficacy of Disease Modifying Therapies in Progressive MS and How Immune Senescence May Explain Their Failure
Abstract
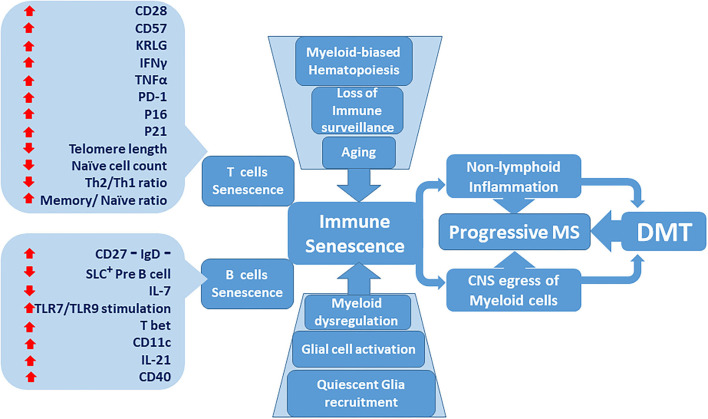
The advent of disease modifying therapies (DMT) in the past two decades has been the cornerstone of successful clinical management of multiple sclerosis (MS). Despite the great strides made in reducing the relapse frequency and occurrence of new signal changes on neuroimaging in patients with relapsing remitting MS (RRMS) by approved DMT, it has been challenging to demonstrate their effectiveness in non-active secondary progressive MS (SPMS) and primary progressive MS (PPMS) disease phenotypes. The dichotomy of DMT effectiveness between RRMS and progressive MS informs on distinct pathogeneses of the different MS phenotypes. Conversely, factors that render patients with progressive MS resistant to therapy are not understood. Thus far, age has emerged as the main correlate of the transition from RRMS to SPMS. Whether it is aging and age-related factors or the underlying immune senescence that qualitatively alter immune responses as the disease transitions to SPMS, that diminish DMT effectiveness, or both, is currently not known. Here, we will discuss the role of immune senescence on different arms of the immune system, and how it may explain relative DMT resistance.
Keywords: adaptive immunity; disease modifying therapies; immunosenescence; innate immunity; multiple sclerosis; progressive multiple sclerosis.
Copyright © 2022 Manouchehri, Salinas, Rabi Yeganeh, Pitt, Hussain and Stuve.
Conflict of interest statement
OS serves on the editorial boards of Therapeutic Advances in Neurological Disorders, has served on data monitoring committees for Genentech-Roche, Pfizer, Novartis, and TG Therapeutics without monetary compensation, has advised EMD Serono, Celgene, Genentech, Genzyme, TG Therapeutics, and VYNE, receives grant support from EMD Serono and Exalys, was a 2021 recipient of a Grant for Multiple Sclerosis Innovation (GMSI), Merck KGaA, and was funded by a Merit Review grant (federal award document number (FAIN) BX005664-01 from the United States (U.S.) Department of Veterans Affairs, Biomedical Laboratory Research and Development). The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous