

Prevalence of intellectual disability in India: A meta-analysis
- PMID: 35433303
- PMCID: PMC8985497
- DOI: 10.5409/wjcp.v11.i2.206
Prevalence of intellectual disability in India: A meta-analysis
Abstract
Background: Burden due to intellectual disability (ID) is only third to the depressive disorders and anxiety disorders in India. This national burden significantly contributes to the global burden of ID and hence one has to think globally and act locally to reduce this burden. At its best the collective prevalence of ID is in the form of narrative reviews. There is an urgent need to document the summary prevalence of ID to enhance further policymaking, national programs and resource allocation.
Aim: To establish the summary prevalence of ID during the past 60 years in India.
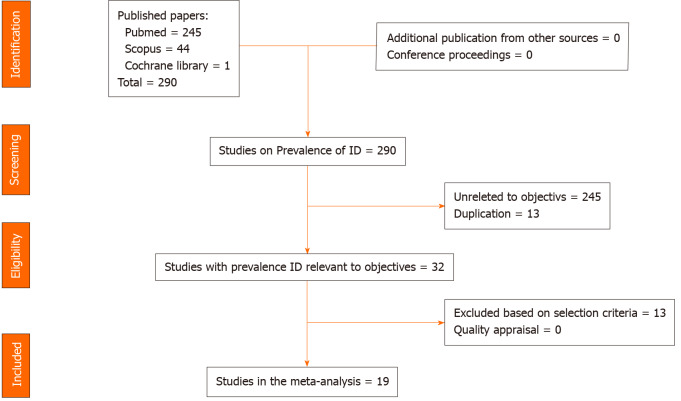
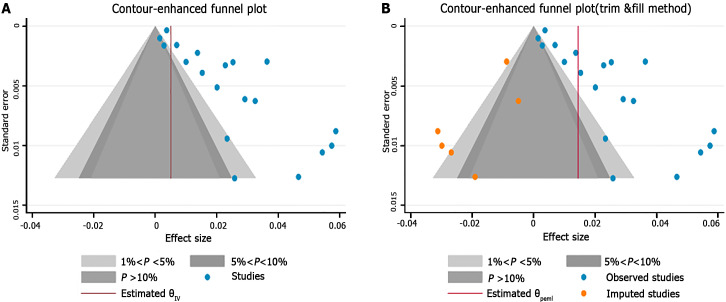
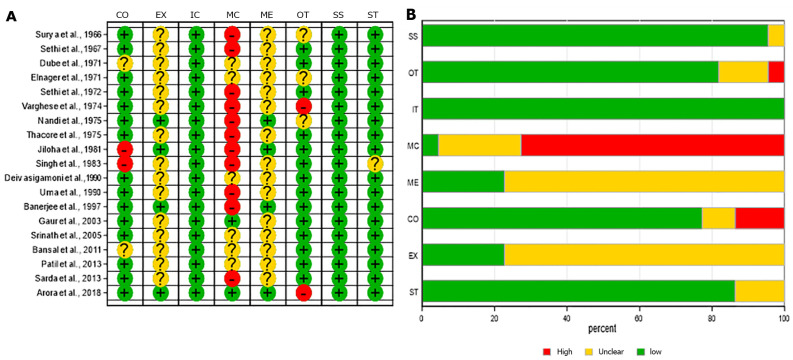
Methods: Two researchers independently and electronically searched PubMed, Scopus, and the Cochrane library from January 1961 to December 2020 using appropriate search terms. Two other investigators extracted the study design, setting, participant characteristics, and measures used to identify ID. Two other researchers appraised the quality of the studies using the Joanna Briggs Institute critical appraisal format for Prevalence Studies. Funnel plot and Egger's regression test were used to ascertain the publication and small study effect on the prevalence. To evaluate the summary prevalence of ID, we used the random effects model with arcsine square-root transformation. Heterogeneity of I 2 ≥ 50% was considered substantial and we determined the heterogeneity with meta-regression. The analyses were performed using STATA (version 16).
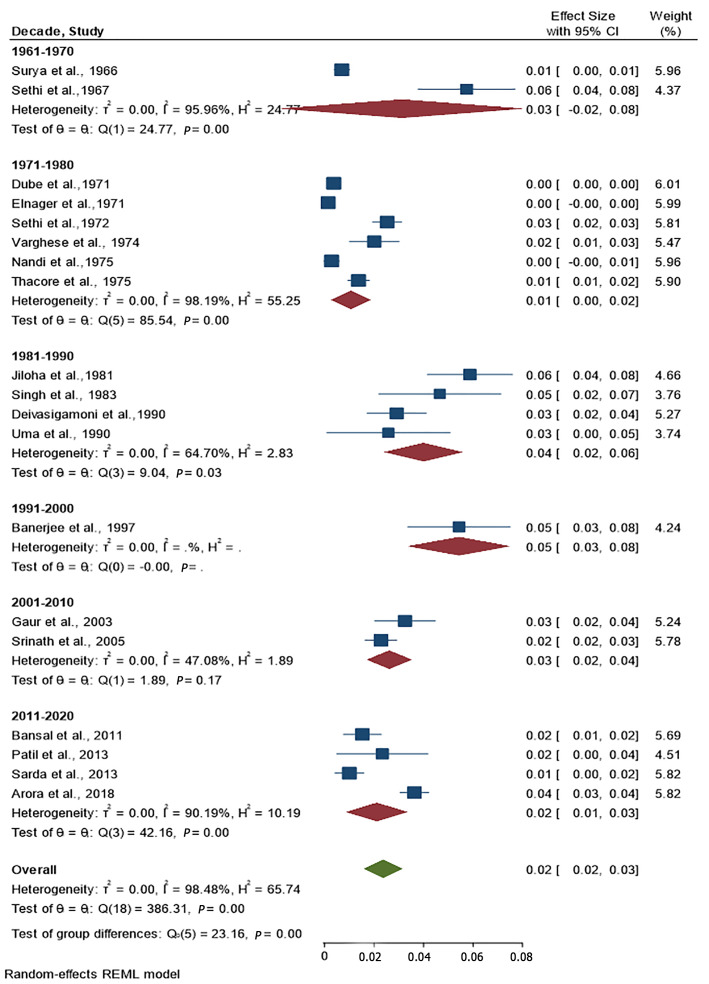
Results: Nineteen studies were included in the meta-analysis. There was publication bias; the trim-and-fill method was used to further ascertain bias. Concerns with control of confounders and the reliable measure of outcome were noted in the critical appraisal. The summary prevalence of ID was 2% [(95%CI: 2%, 3%); I 2 = 98%] and the adjusted summary prevalence was 1.4%. Meta-regression demonstrated that age of the participants was statistically significantly related to the prevalence; other factors did not influence the prevalence or heterogeneity.
Conclusion: The summary prevalence of ID in India was established to be 2% taking into consideration the individual prevalence studies over the last six decades. This knowledge should improve the existing disability and mental health policies, national programs and service delivery to reduce the national and global burden associated with ID.
Keywords: Children and adolescents; India; Intellectual disability; Meta-analysis; Prevalence.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no conflict of interest.
Figures
References
-
- Shidhaye R. Unburden mental health in India: it's time to act now. Lancet Psychiatry. 2020;7:111–112. - PubMed
-
- Girimaji SC, Srinath S. Perspectives of intellectual disability in India: epidemiology, policy, services for children and adults. Curr Opin Psychiatry. 2010;23:441–446. - PubMed
-
- Lal N, Sethi BB. Estimate of mental ill health in children of an urban community. Indian J Pediatr. 1977;44:55–64. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
