

Improving Pediatric/Neonatology Residents' Newborn Resuscitation Skills With a Digital Serious Game: DIANA
- PMID: 35433552
- PMCID: PMC9010974
- DOI: 10.3389/fped.2022.842302
Improving Pediatric/Neonatology Residents' Newborn Resuscitation Skills With a Digital Serious Game: DIANA
Abstract
Background: Serious games, and especially digital game based learning (DGBL) methodologies, have the potential to strengthen classic learning methodology in all medical procedures characterized by a flowchart (e.g., neonatal resuscitation algorithm). However, few studies have compared short- and long-term knowledge retention in DGBL methodologies with a control group undergoing specialist training led by experienced operators. In particular, resident doctors' learning still has limited representation in simulation-based education literature.
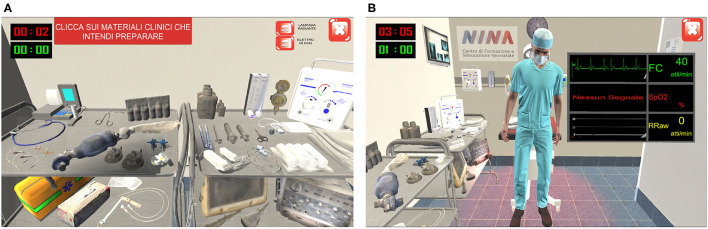
Objective: A serious computer game DIANA (DIgital Application in Newborn Assessment) was developed, according to newborn resuscitation algorithm, to train pediatric/neonatology residents in neonatal resuscitation algorithm knowledge and implementation (from procedure knowledge to ventilation/chest compressions rate). We analyzed user learning curves after each session and compared knowledge retention against a classic theoretical teaching session.
Methods: Pediatric/neonatology residents of the Azienda Ospedaliera Universitaria Pisana (AOUP) were invited to take part in the study and were split into a game group or a control group; both groups were homogeneous in terms of previous training and baseline scores. The control group attended a classic 80 min teaching session with a neonatal trainer, while game group participants played four 20 min sessions over four different days. Three written tests (pre/immediately post-training and at 28 days) were used to evaluate and compare the two groups' performances.
Results: Forty-eight pediatric/neonatology residents participated in the study. While classic training by a neonatal trainer demonstrated an excellent effectiveness in short/long-term knowledge retention, DGBL methodology proved to be equivalent or better. Furthermore, after each game session, DGBL score improved for both procedure knowledge and ventilation/chest compressions rate.
Conclusions: In this study, DGBL was as effective as classic specialist training for neonatal resuscitation in terms of both algorithm memorization and knowledge retention. User appreciation for the methodology and ease of administration, including remotely, support the use of DGBL methodologies for pediatric/neonatology residents education.
Keywords: DGBL; digital games; healthcare education; memory and retention; neonatal resuscitation; newborn infants; serious game; technology-enhanced training or learning.
Copyright © 2022 Bardelli, Del Corso, Ciantelli, Del Pistoia, Lorenzoni, Fossati, Scaramuzzo and Cuttano.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures












References
-
- Wyckoff MH, Wyllie J, Aziz K, de Almeida MF, Fabres J, Fawke J, et al. . Neonatal life support: 2020 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Circulation. (2020) 142(16 Suppl. 1):S185–221. 10.1542/peds.2020-038505C - DOI - PubMed
-
- Pesare E, Roselli T, Corriero N, Rossano V. Game-based learning and gamification to promote engagement and motivation in medical learning contexts. Smart Learn Environ. (2016) 3:1–21. 10.1186/s40561-016-0028-0 - DOI
LinkOut - more resources
Full Text Sources