

Inflammatory responses in the placenta upon SARS-CoV-2 infection late in pregnancy
- PMID: 35434541
- PMCID: PMC8996470
- DOI: 10.1016/j.isci.2022.104223
Inflammatory responses in the placenta upon SARS-CoV-2 infection late in pregnancy
Abstract
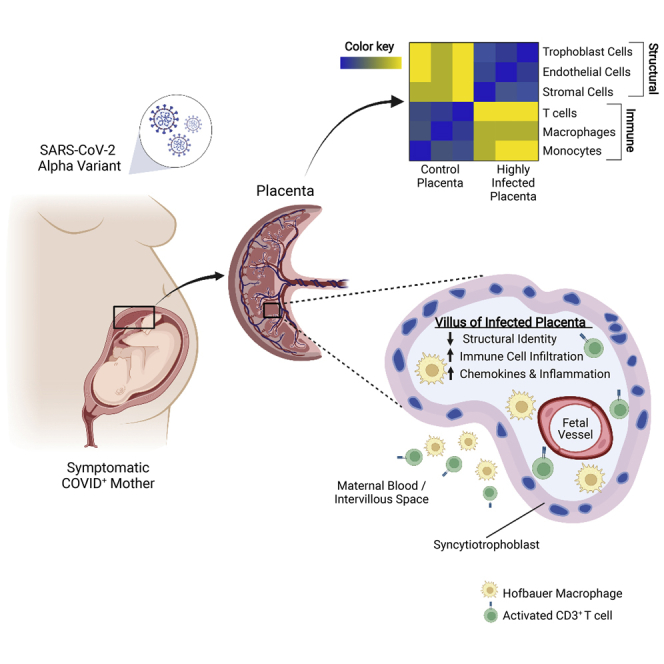
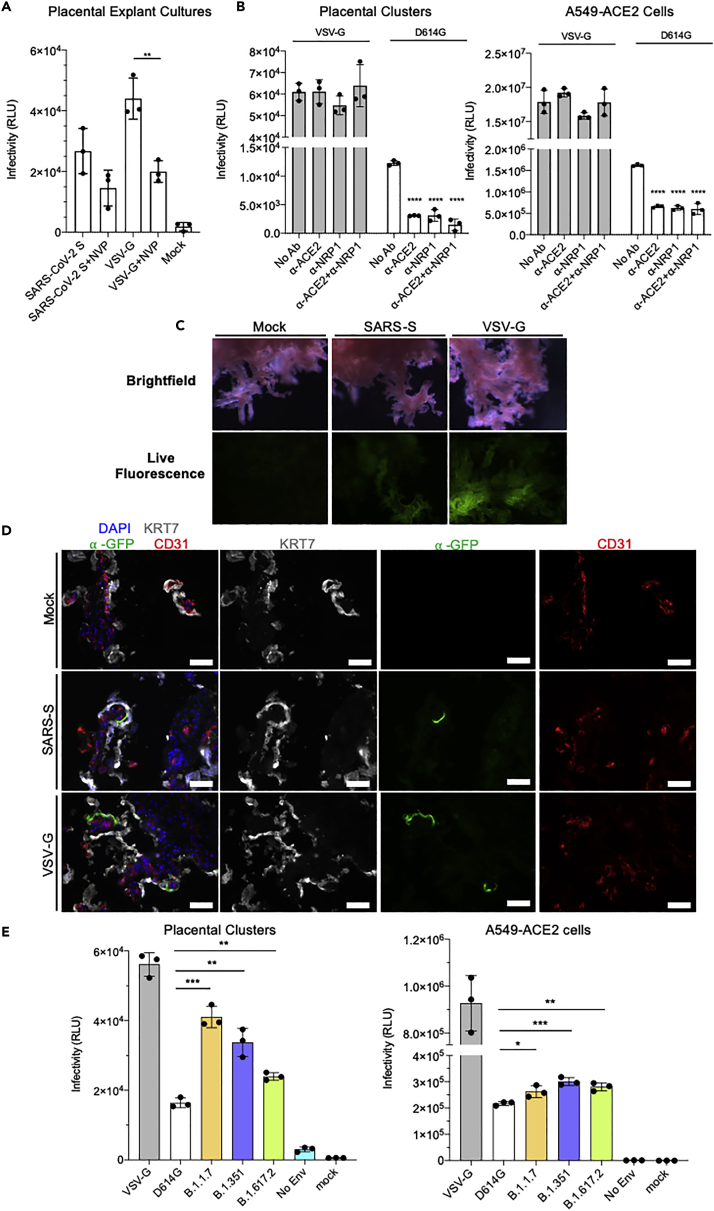
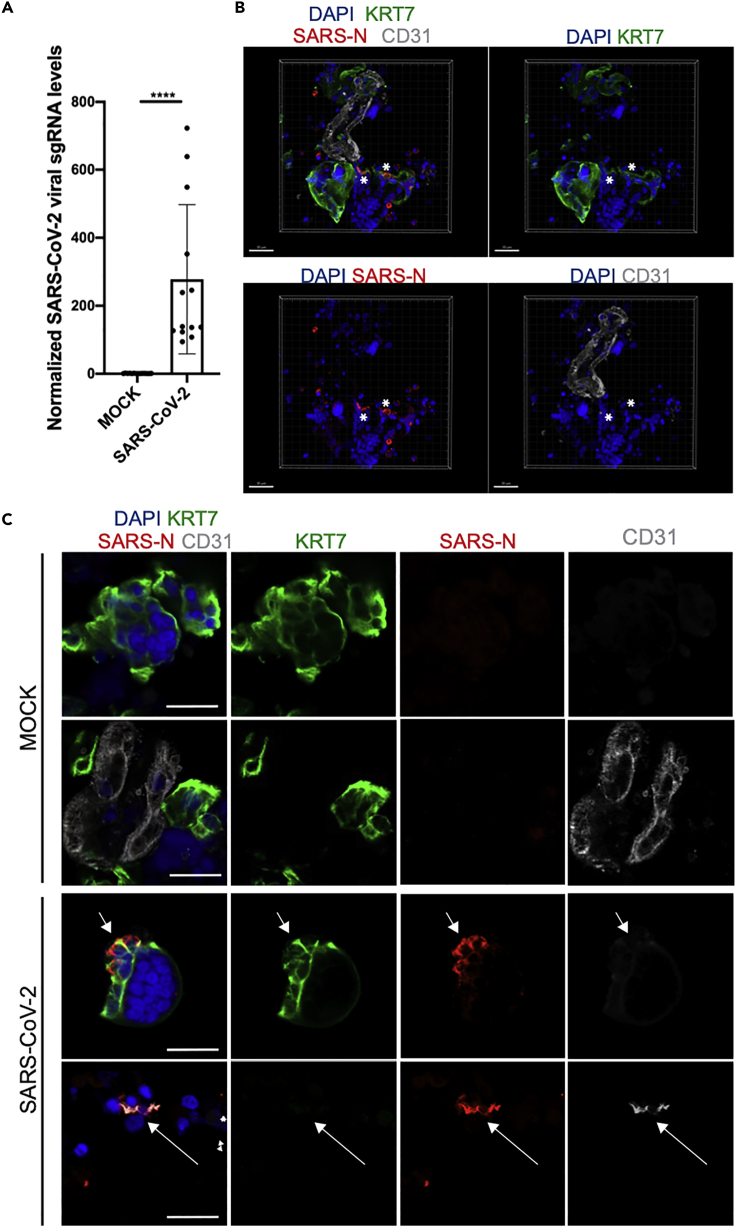
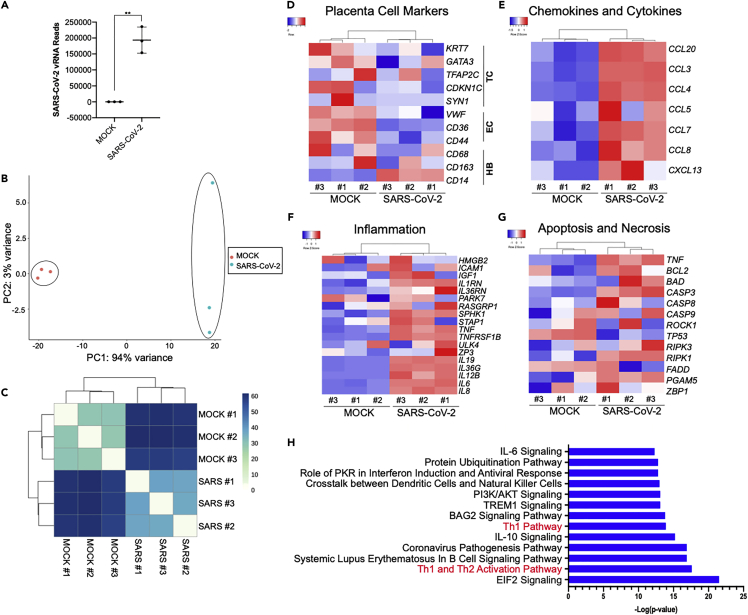
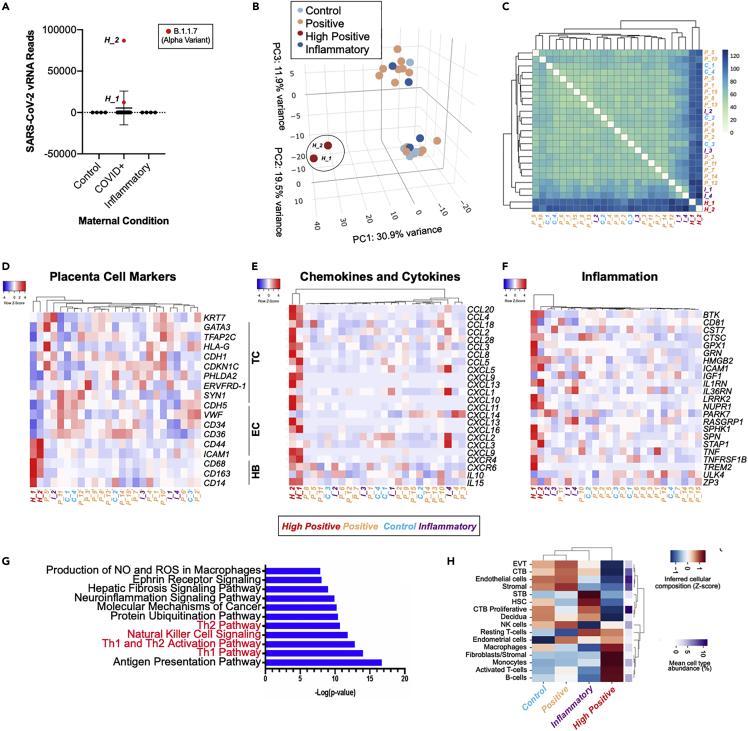
The effect of SARS-CoV-2 infection on placental function is not well understood. Analysis of placentas from women who tested positive at delivery showed SARS-CoV-2 genomic and subgenomic RNA in 22 out of 52 placentas. Placentas from two mothers with symptomatic COVID-19 whose pregnancies resulted in adverse outcomes for the fetuses contained high levels of viral Alpha variant RNA. The RNA was localized to the trophoblasts that cover the fetal chorionic villi in direct contact with maternal blood. The intervillous spaces and villi were infiltrated with maternal macrophages and T cells. Transcriptome analysis showed an increased expression of chemokines and pathways associated with viral infection and inflammation. Infection of placental cultures with live SARS-CoV-2 and spike protein-pseudotyped lentivirus showed infection of syncytiotrophoblast and, in rare cases, endothelial cells mediated by ACE2 and Neuropilin-1. Viruses with Alpha, Beta, and Delta variant spikes infected the placental cultures at significantly greater levels.
Keywords: Health sciences; Immunology; Transcriptomics.
© 2022 The Author(s).
Conflict of interest statement
O.E. is a scientific advisor and equity holder in Freenome, Owkin, Volastra Therapeutics, and One Three Biotech. R.E.S. is on the scientific advisory board of Miromatrix Inc and is a consultant and speaker for Alnylam Inc.
Figures


Update of
-
SARS-CoV-2 Infects Syncytiotrophoblast and Activates Inflammatory Responses in the Placenta.bioRxiv [Preprint]. 2021 Jun 17:2021.06.01.446676. doi: 10.1101/2021.06.01.446676. bioRxiv. 2021. Update in: iScience. 2022 May 20;25(5):104223. doi: 10.1016/j.isci.2022.104223. PMID: 34100019 Free PMC article. Updated. Preprint.
References
-
- Alamar I., Abu-Arja M.H., Heyman T., Roberts D.J., Desai N., Narula P., Dygulska B. A possible case of vertical transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in a newborn with positive placental in situ hybridization of SARS-CoV-2 RNA. J. Pediatr. Infect. Dis. Soc. 2020;9:636–639. - PMC - PubMed
-
- Arad A., Nammouz S., Nov Y., Ohel G., Bejar J., Vadasz Z. The expression of neuropilin-1 in human placentas from normal and preeclamptic pregnancies. Int. J. Gynecol. Pathol. 2017;36:42–49. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
