

Infiltrative growth pattern of prostate cancer is associated with lower uptake on PSMA PET and reduced diffusion restriction on mpMRI
- PMID: 35435496
- PMCID: PMC9399036
- DOI: 10.1007/s00259-022-05787-9
Infiltrative growth pattern of prostate cancer is associated with lower uptake on PSMA PET and reduced diffusion restriction on mpMRI
Abstract
Purpose: Recently, a significant association was shown between novel growth patterns on histopathology of prostate cancer (PCa) and prostate-specific membrane antigen (PSMA) uptake on [68Ga]PSMA-PET. It is the aim of this study to evaluate the association between these growth patterns and ADC (mm2/1000 s) values in comparison to [68Ga]PSMA uptake on PET/MRI.
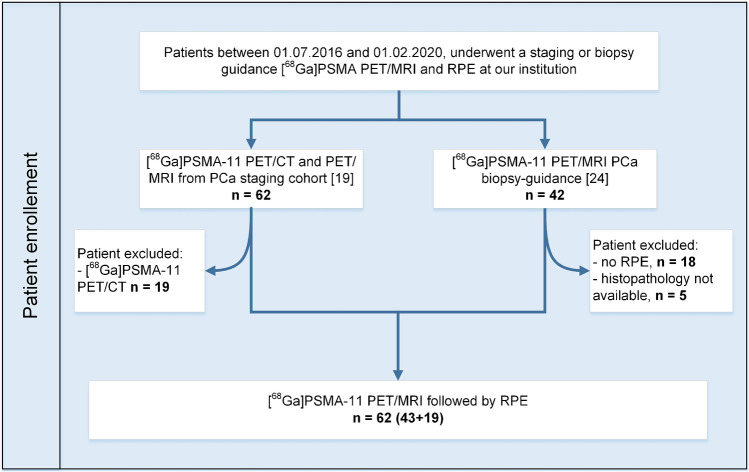
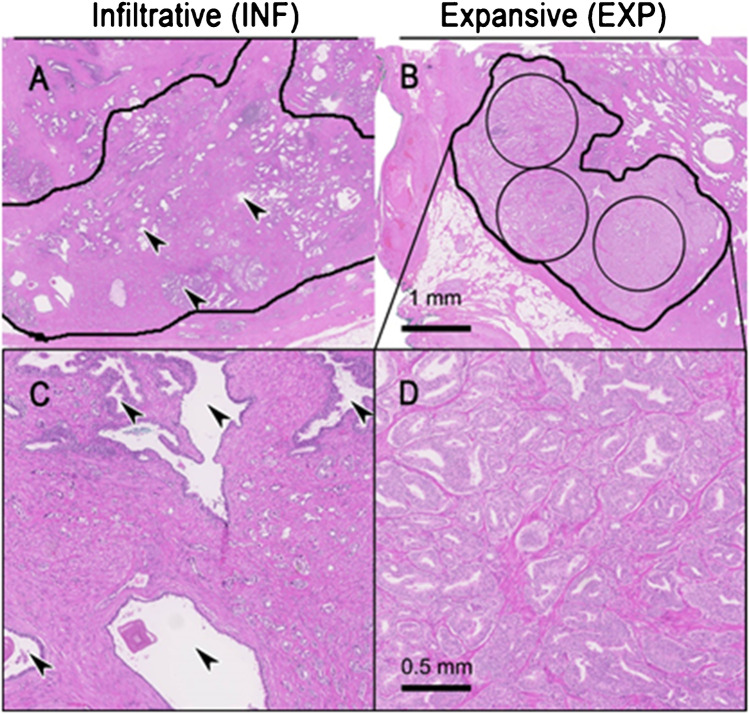
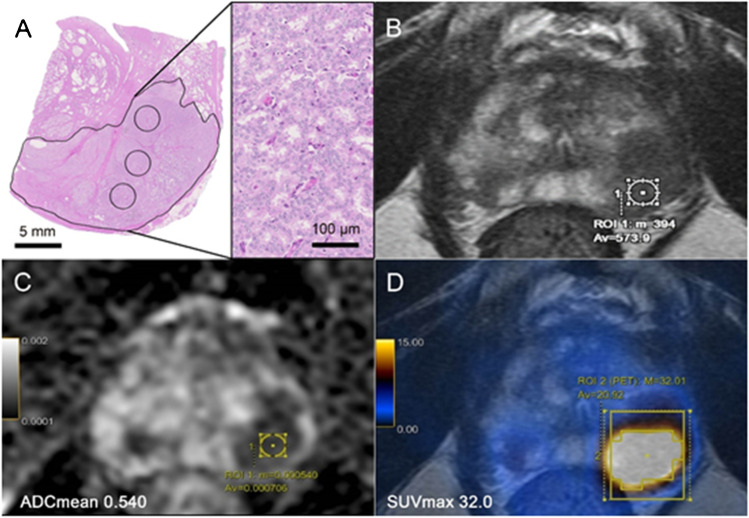
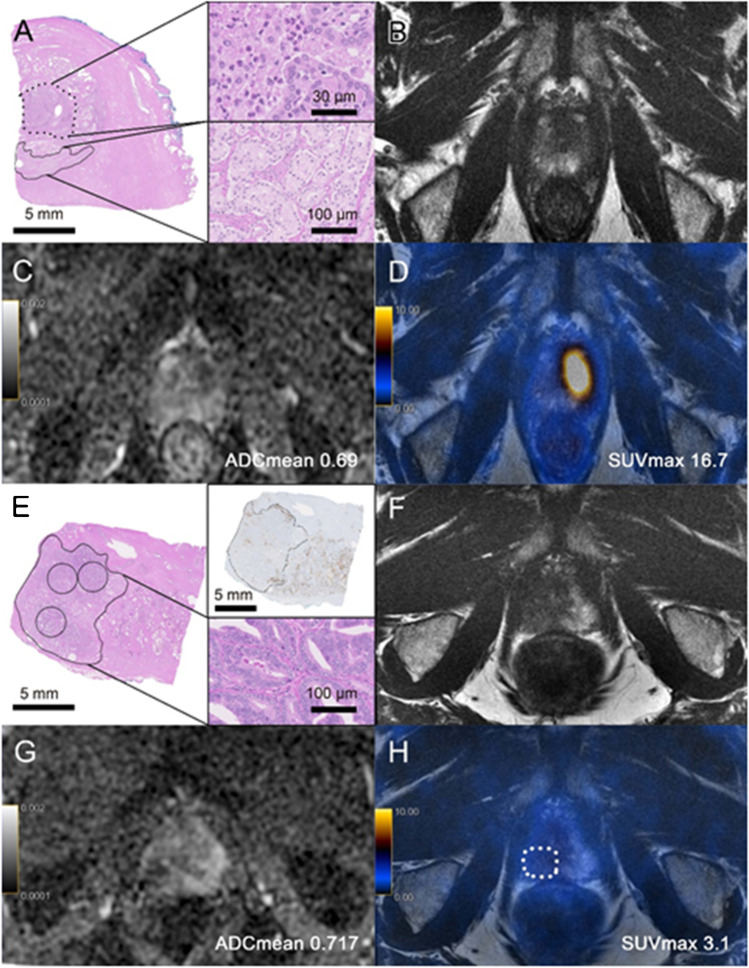
Methods: We retrospectively evaluated patients who underwent [68Ga]PSMA PET/MRI for staging or biopsy guidance, followed by radical prostatectomy at our institution between 07/2016 and 01/2020. The dominant lesion per patient was selected based on histopathology and correlated to PET/MRI in a multidisciplinary meeting, and quantified using SUVmax for PSMA uptake and ADCmean for diffusion restriction. PCa growth pattern was classified as expansive (EXP) or infiltrative (INF) according to its properties of forming a tumoral mass or infiltrating diffusely between benign glands by two independent pathologists. Furthermore, the corresponding WHO2016 ISUP tumor grade was evaluated. The t test was used to compare means, Pearson's test for categorical correlation, Cohen's kappa test for interrater agreement, and ROC curve to determine the best cutoff.
Results: Sixty-two patients were included (mean PSA 11.7 ± 12.5). The interrater agreement between both pathologists was almost perfect with κ = 0.81. While 25 lesions had an EXP-growth with an ADCmean of 0.777 ± 0.109, 37 showed an INF-growth with a significantly higher ADCmean of 1.079 ± 0.262 (p < 0.001). We also observed a significant difference regarding PSMA SUVmax for the EXP-growth (19.2 ± 10.9) versus the INF-growth (9.4 ± 6.2, p < 0.001). Within the lesions encompassing the EXP- or the INF-growth, no significant correlation between the ISUP groups and ADCmean could be observed (p = 0.982 and p = 0.861, respectively).
Conclusion: PCa with INF-growth showed significantly lower SUVmax and higher ADCmean values compared to PCa with EXP-growth. Within the growth groups, ADCmean values were independent from ISUP grading.
Keywords: Diffusion-weighted imaging; MRI; PSMA PET/MRI; Prostate cancer; Radical prostatectomy.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Schoots IG, Roobol MJ, Nieboer D, Bangma CH, Steyerberg EW, Hunink MG. Magnetic resonance imaging-targeted biopsy may enhance the diagnostic accuracy of significant prostate cancer detection compared to standard transrectal ultrasound-guided biopsy: a systematic review and meta-analysis. Eur Urol. 2015;68:438–450. doi: 10.1016/j.eururo.2014.11.037. - DOI - PubMed
-
- Turkbey B, Rosenkrantz AB, Haider MA, et al. Prostate imaging reporting and data system version 2.1: 2019 update of prostate imaging reporting and data system version 2. Eur Urol. 2019;76:340–351. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
