

Assessment of Awake Prone Positioning in Hospitalized Adults With COVID-19: A Nonrandomized Controlled Trial
- PMID: 35435937
- PMCID: PMC9016608
- DOI: 10.1001/jamainternmed.2022.1070
Assessment of Awake Prone Positioning in Hospitalized Adults With COVID-19: A Nonrandomized Controlled Trial
Abstract
Importance: Awake prone positioning may improve hypoxemia among patients with COVID-19, but whether it is associated with improved clinical outcomes remains unknown.
Objective: To determine whether the recommendation of awake prone positioning is associated with improved outcomes among patients with COVID-19-related hypoxemia who have not received mechanical ventilation.
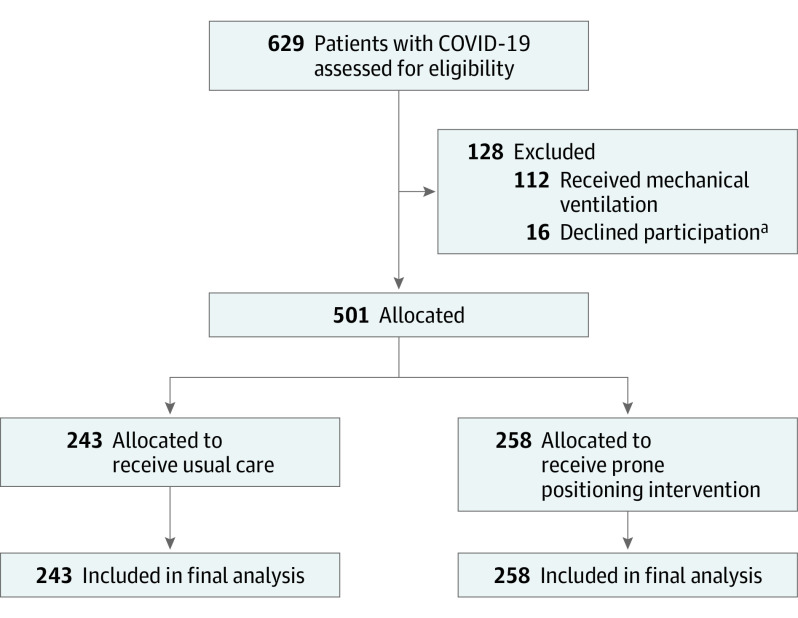
Design, setting, and participants: This pragmatic nonrandomized controlled trial was conducted at 2 academic medical centers (Vanderbilt University Medical Center and NorthShore University HealthSystem) during the COVID-19 pandemic. A total of 501 adult patients with COVID-19-associated hypoxemia who had not received mechanical ventilation were enrolled from May 13 to December 11, 2020.
Interventions: Patients were assigned 1:1 to receive either the practitioner-recommended awake prone positioning intervention (intervention group) or usual care (usual care group).
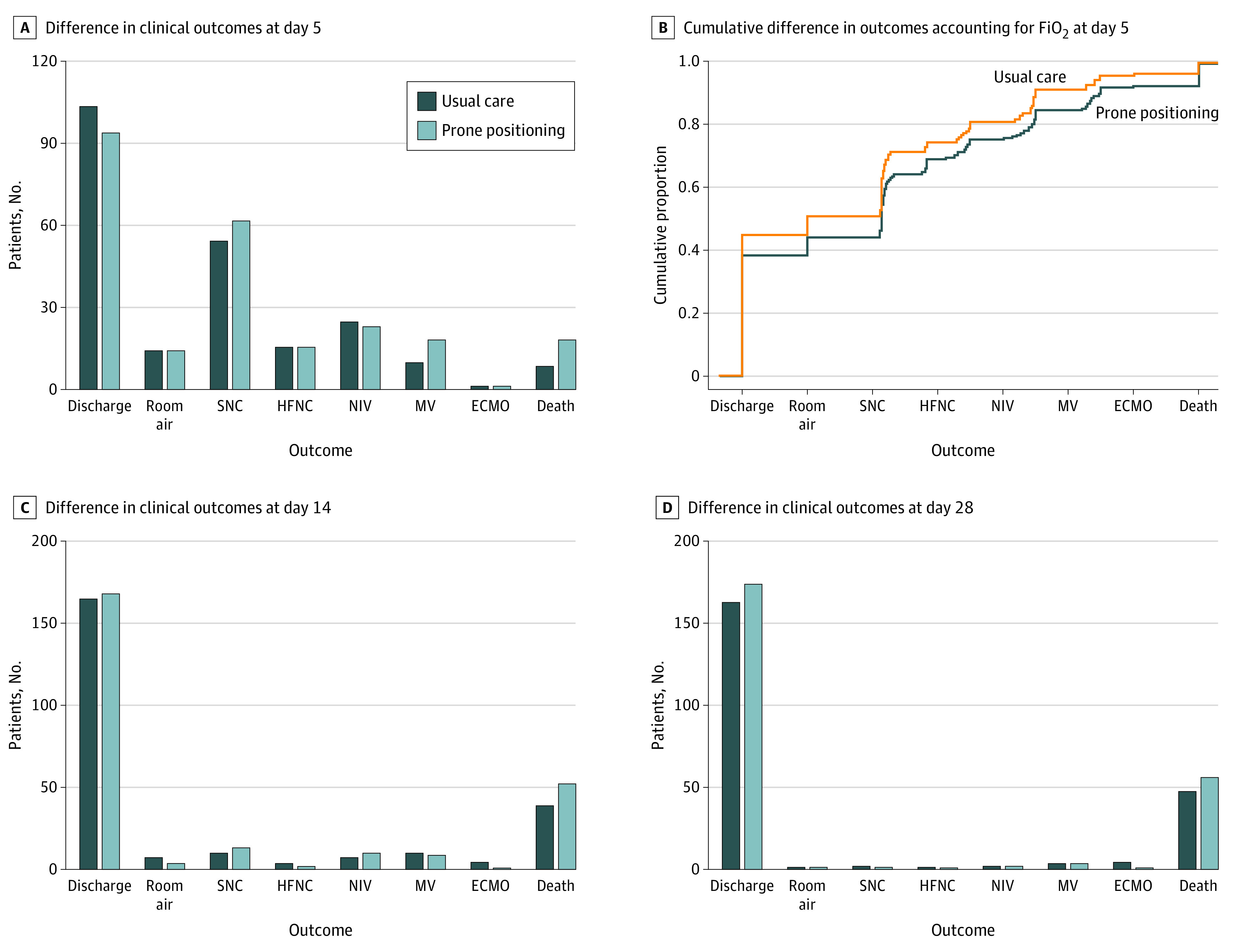
Main outcomes and measures: Primary outcome analyses were performed using a bayesian proportional odds model with covariate adjustment for clinical severity ranking based on the World Health Organization ordinal outcome scale, which was modified to highlight the worst level of hypoxemia on study day 5.
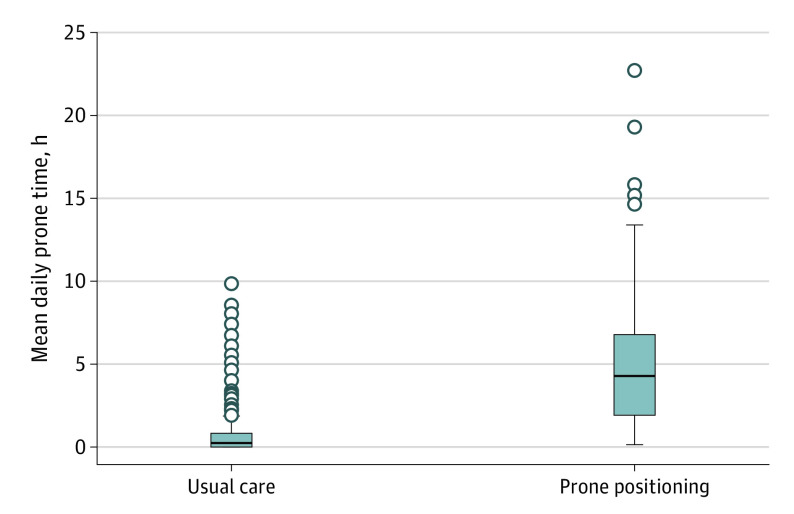
Results: A total of 501 patients (mean [SD] age, 61.0 [15.3] years; 284 [56.7%] were male; and most [417 (83.2%)] were self-reported non-Hispanic or non-Latinx) were included. Baseline severity was comparable between the intervention vs usual care groups, with 170 patients (65.9%) vs 162 patients (66.7%) receiving oxygen via standard low-flow nasal cannula, 71 patients (27.5%) vs 62 patients (25.5%) receiving oxygen via high-flow nasal cannula, and 16 patients (6.2%) vs 19 patients (7.8%) receiving noninvasive positive-pressure ventilation. Nursing observations estimated that patients in the intervention group spent a median of 4.2 hours (IQR, 1.8-6.7 hours) in the prone position per day compared with 0 hours (IQR, 0-0.7 hours) per day in the usual care group. On study day 5, the bayesian posterior probability of the intervention group having worse outcomes than the usual care group on the modified World Health Organization ordinal outcome scale was 0.998 (posterior median adjusted odds ratio [aOR], 1.63; 95% credibility interval [CrI], 1.16-2.31). However, on study days 14 and 28, the posterior probabilities of harm were 0.874 (aOR, 1.29; 95% CrI, 0.84-1.99) and 0.673 (aOR, 1.12; 95% CrI, 0.67-1.86), respectively. Exploratory outcomes (progression to mechanical ventilation, length of stay, and 28-day mortality) did not differ between groups.
Conclusions and relevance: In this nonrandomized controlled trial, prone positioning offered no observed clinical benefit among patients with COVID-19-associated hypoxemia who had not received mechanical ventilation. Moreover, there was substantial evidence of worsened clinical outcomes at study day 5 among patients recommended to receive the awake prone positioning intervention, suggesting potential harm.
Trial registration: ClinicalTrials.gov Identifier: NCT04359797.
Conflict of interest statement
Figures
Comment in
-
Prone Positioning for Nonintubated Patients With COVID-19-Potential Dangers of Extrapolation and Intermediate Outcome Variables.JAMA Intern Med. 2022 Jun 1;182(6):622-623. doi: 10.1001/jamainternmed.2022.1086. JAMA Intern Med. 2022. PMID: 35435933 No abstract available.
-
Awake Prone Positioning in COVID-19: Signal or Noise?JAMA Intern Med. 2022 Sep 1;182(9):1013. doi: 10.1001/jamainternmed.2022.3115. JAMA Intern Med. 2022. PMID: 35913712 No abstract available.
-
Awake Prone Positioning in COVID-19: Signal or Noise?-Reply.JAMA Intern Med. 2022 Sep 1;182(9):1014-1015. doi: 10.1001/jamainternmed.2022.3112. JAMA Intern Med. 2022. PMID: 35913713 No abstract available.
-
Awake Prone Positioning in COVID-19: Signal or Noise?JAMA Intern Med. 2022 Sep 1;182(9):1013-1014. doi: 10.1001/jamainternmed.2022.3575. JAMA Intern Med. 2022. PMID: 35913730 No abstract available.
References
-
- World Health Organization . Coronavirus disease (COVID-19). World Health Organization; 2020. Accessed August 21, 2020. https://www.who.int/health-topics/coronavirus
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
