

The diagnostic value of nasal microbiota and clinical parameters in a multi-parametric prediction model to differentiate bacterial versus viral infections in lower respiratory tract infections
- PMID: 35436301
- PMCID: PMC9015155
- DOI: 10.1371/journal.pone.0267140
The diagnostic value of nasal microbiota and clinical parameters in a multi-parametric prediction model to differentiate bacterial versus viral infections in lower respiratory tract infections
Abstract
Background: The ability to accurately distinguish bacterial from viral infection would help clinicians better target antimicrobial therapy during suspected lower respiratory tract infections (LRTI). Although technological developments make it feasible to rapidly generate patient-specific microbiota profiles, evidence is required to show the clinical value of using microbiota data for infection diagnosis. In this study, we investigated whether adding nasal cavity microbiota profiles to readily available clinical information could improve machine learning classifiers to distinguish bacterial from viral infection in patients with LRTI.
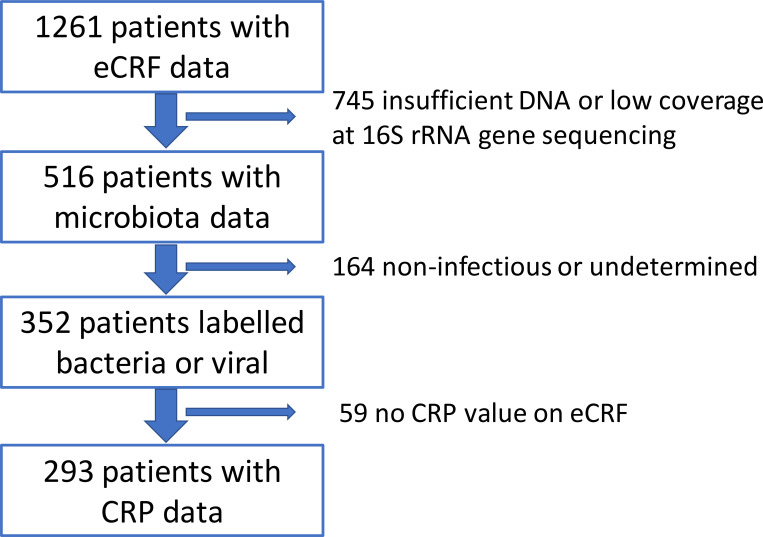
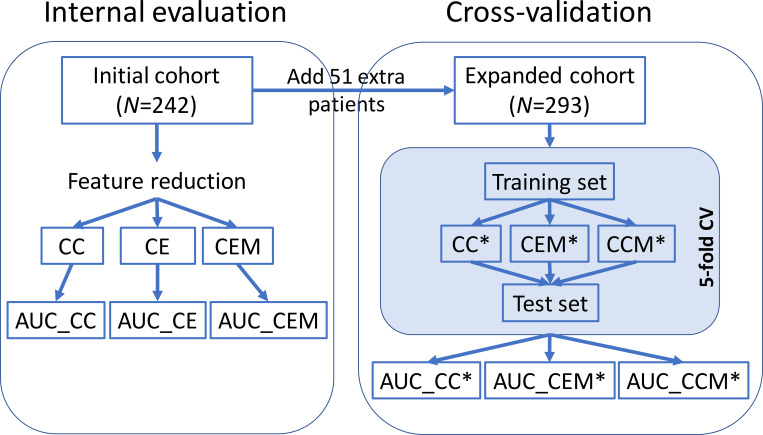
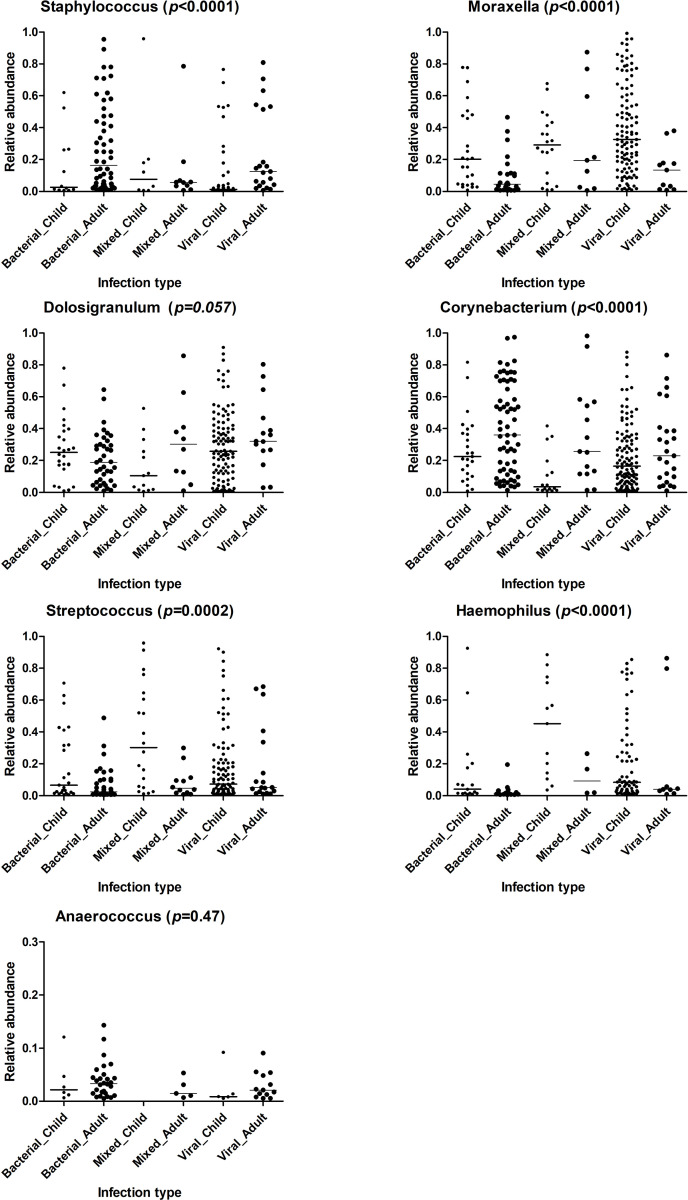
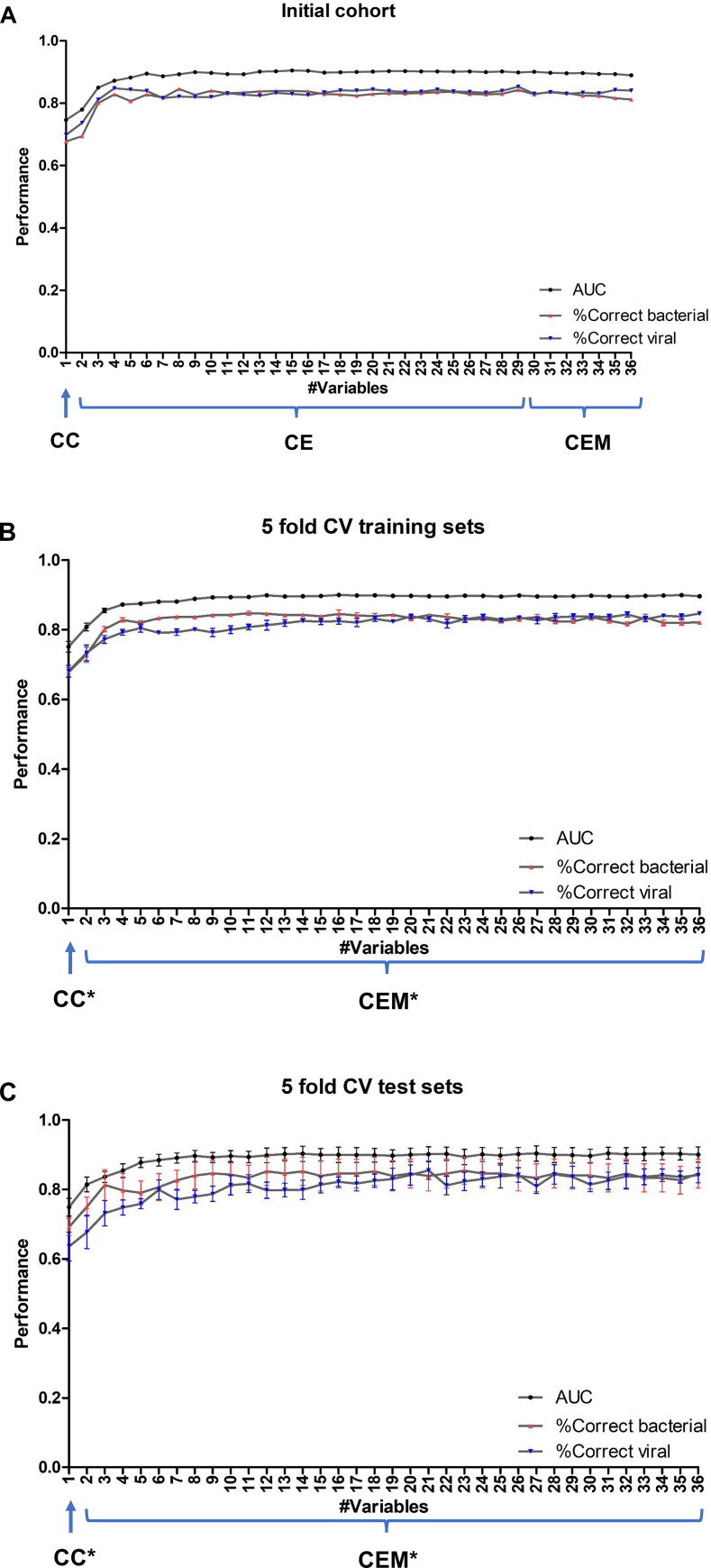
Results: Various multi-parametric Random Forests classifiers were evaluated on the clinical and microbiota data of 293 LRTI patients for their prediction accuracies to differentiate bacterial from viral infection. The most predictive variable was C-reactive protein (CRP). We observed a marginal prediction improvement when 7 most prevalent nasal microbiota genera were added to the CRP model. In contrast, adding three clinical variables, absolute neutrophil count, consolidation on X-ray, and age group to the CRP model significantly improved the prediction. The best model correctly predicted 85% of the 'bacterial' patients and 82% of the 'viral' patients using 13 clinical and 3 nasal cavity microbiota genera (Staphylococcus, Moraxella, and Streptococcus).
Conclusions: We developed high-accuracy multi-parametric machine learning classifiers to differentiate bacterial from viral infections in LRTI patients of various ages. We demonstrated the predictive value of four easy-to-collect clinical variables which facilitate personalized and accurate clinical decision-making. We observed that nasal cavity microbiota correlate with the clinical variables and thus may not add significant value to diagnostic algorithms that aim to differentiate bacterial from viral infections.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Marshall DC, Goodson RJ, Xu YW, Komorowski M, Shalhoub J, Maruthappu M, et al.. Trends in mortality from pneumonia in the Europe union: a temporal analysis of the European detailed mortality database between 2001 and 2014. Resp Res. 2018;19. doi: 10.1186/s12931-018-0781-4 WOS:000431832800001. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
