

Safety and immunogenicity of SpikoGen®, an Advax-CpG55.2-adjuvanted SARS-CoV-2 spike protein vaccine: a phase 2 randomized placebo-controlled trial in both seropositive and seronegative populations
- PMID: 35436611
- PMCID: PMC9012510
- DOI: 10.1016/j.cmi.2022.04.004
Safety and immunogenicity of SpikoGen®, an Advax-CpG55.2-adjuvanted SARS-CoV-2 spike protein vaccine: a phase 2 randomized placebo-controlled trial in both seropositive and seronegative populations
Abstract
Objective: We aimed to investigate the immunogenicity and safety of SpikoGen®, a subunit COVID-19 vaccine composed of a recombinant prefusion-stabilized SARS-CoV-2 spike protein combined with the Advax-CpG55.2™ adjuvant, in seronegative and seropositive populations as primary vaccination.
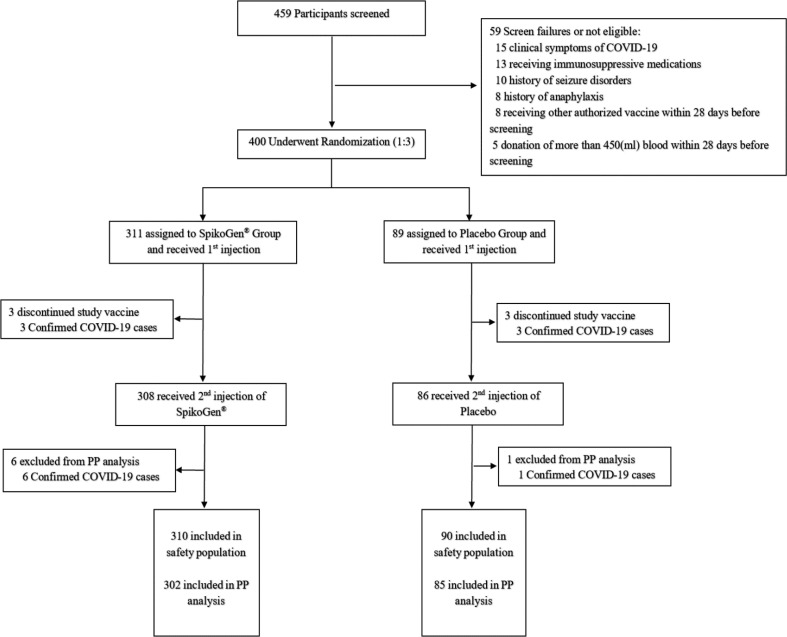
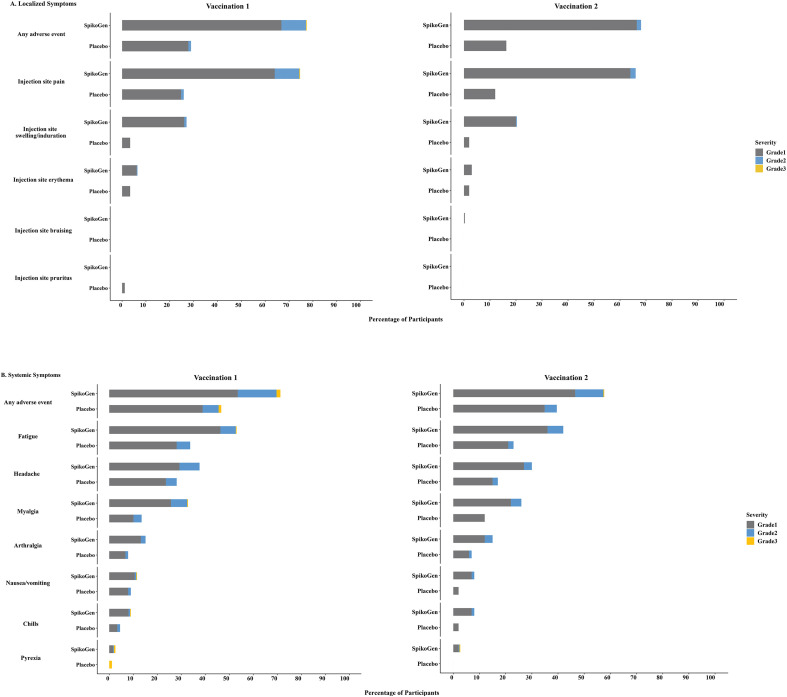
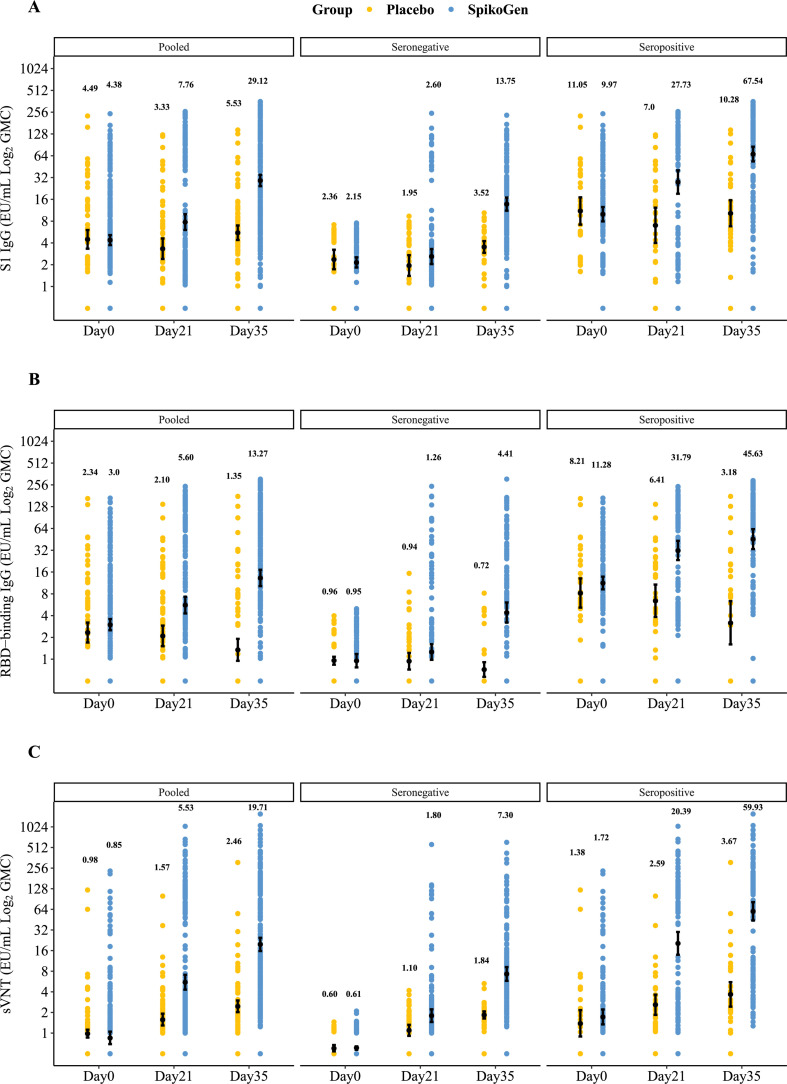
Methods: This randomized, placebo-controlled, double-blind phase 2 trial was conducted on 400 participants randomized 3:1 to receive two doses of 25 μg of SpikoGen® 3 weeks apart or the placebo. The primary safety outcomes were the incidence of solicited adverse events up to 7 days after each dose and unsolicited adverse events up to 28 days after the second dose. The primary immunogenicity outcomes were seroconversion against the S1 protein and the geometric mean concentration of S1 antibodies by days 21 and 35.
Results: The SpikoGen® vaccine was well tolerated and no serious adverse events were recorded. The most common solicited adverse events were injection site pain and fatigue, largely graded as mild and transient. By day 35 (2 weeks post second dose), the seroconversion rate against S1 was 63.55 (95% CI: 57.81-69.01) in the SpikoGen® group versus 7.23 (95% CI: 2.7-15.07) in the placebo group. The geometric mean concentration of S1 antibodies was 29.12 (95% CI: 24.32-34.87) in the SpikoGen® group versus 5.53 (95% CI: 4.39-6.97) in the placebo group. Previously infected seropositive volunteers showed a large SARS-CoV-2 humoral response after a single SpikoGen® dose.
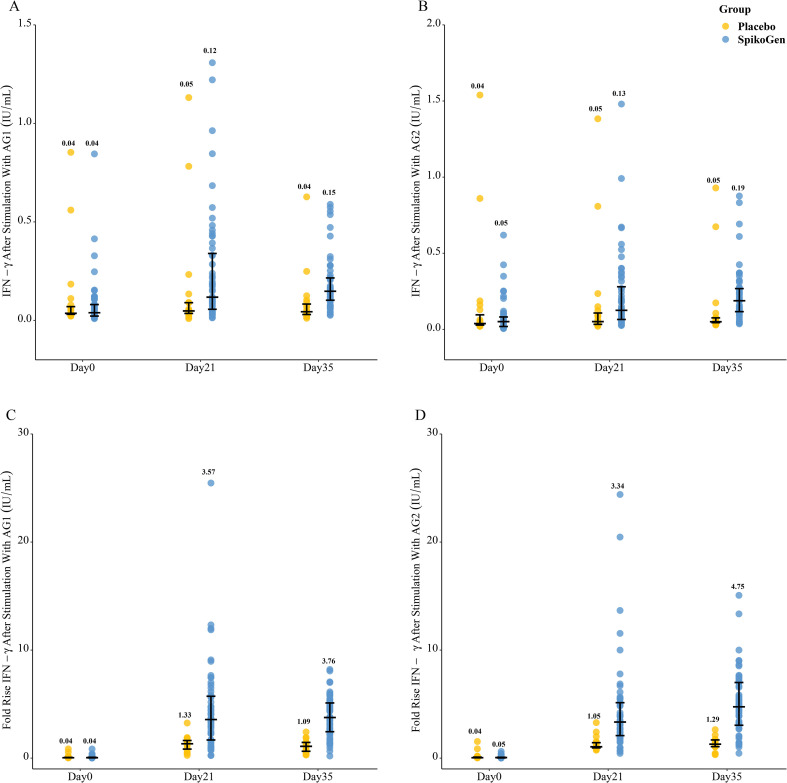
Discussion: SpikoGen® had an acceptable safety profile and induced promising humoral and cellular immune responses against SARS-CoV-2.
Keywords: Advax-CpG; COVID-19; Phase 2; SARS-CoV-2; SpikoGen; Subunit protein vaccine.
Copyright © 2022 European Society of Clinical Microbiology and Infectious Diseases. Published by Elsevier Ltd. All rights reserved.
Figures
Similar articles
-
Immunogenicity and safety of SpikoGen®, an adjuvanted recombinant SARS-CoV-2 spike protein vaccine as a homologous and heterologous booster vaccination: A randomized placebo-controlled trial.Immunology. 2022 Nov;167(3):340-353. doi: 10.1111/imm.13540. Epub 2022 Jul 13. Immunology. 2022. PMID: 35758850 Free PMC article. Clinical Trial.
-
Immunogenicity and Safety of SpikoGen, an Adjuvanted Recombinant SARS-CoV-2 Spike Protein, as a Heterologous Third Booster Dose in Kidney Transplant Patients: A Single-arm Clinical Trial.Clin Ther. 2022 Dec;44(12):1566-1576. doi: 10.1016/j.clinthera.2022.10.002. Epub 2022 Oct 24. Clin Ther. 2022. PMID: 36402595 Free PMC article. Clinical Trial.
-
Comparative immunogenicity and safety of SpikoGen®, a recombinant SARS-CoV-2 spike protein vaccine in children and young adults: An immuno-bridging clinical trial.Int Immunopharmacol. 2024 Jan 25;127:111436. doi: 10.1016/j.intimp.2023.111436. Epub 2023 Dec 25. Int Immunopharmacol. 2024. PMID: 38147778 Clinical Trial.
-
Clinical development of SpikoGen®, an Advax-CpG55.2 adjuvanted recombinant spike protein vaccine.Hum Vaccin Immunother. 2024 Dec 31;20(1):2363016. doi: 10.1080/21645515.2024.2363016. Epub 2024 Jun 5. Hum Vaccin Immunother. 2024. PMID: 38839044 Free PMC article. Review.
-
Clinical Approach to Post-acute Sequelae After COVID-19 Infection and Vaccination.Cureus. 2023 Nov 21;15(11):e49204. doi: 10.7759/cureus.49204. eCollection 2023 Nov. Cureus. 2023. PMID: 38024037 Free PMC article. Review.
Cited by
-
Plant-derived immuno-adjuvants in vaccines formulation: a promising avenue for improving vaccines efficacy against SARS-CoV-2 virus.Pharmacol Rep. 2022 Dec;74(6):1238-1254. doi: 10.1007/s43440-022-00418-4. Epub 2022 Sep 20. Pharmacol Rep. 2022. PMID: 36125739 Free PMC article. Review.
-
Revolutionizing adjuvant development: harnessing AI for next-generation cancer vaccines.Front Immunol. 2024 Aug 14;15:1438030. doi: 10.3389/fimmu.2024.1438030. eCollection 2024. Front Immunol. 2024. PMID: 39206192 Free PMC article. Review.
-
Adverse events following COVID-19 vaccination: A systematic review and meta-analysis.Int Immunopharmacol. 2022 Aug;109:108906. doi: 10.1016/j.intimp.2022.108906. Epub 2022 May 30. Int Immunopharmacol. 2022. PMID: 35671640 Free PMC article.
-
Lessons Learned from COVID-19 Pandemic Management in Iran; a Commentary.Arch Acad Emerg Med. 2024 Feb 7;12(1):e24. doi: 10.22037/aaem.v12i1.2241. eCollection 2024. Arch Acad Emerg Med. 2024. PMID: 38572222 Free PMC article. No abstract available.
-
COVID-19 Vaccines: Where Did We Stand at the End of 2023?Viruses. 2024 Jan 29;16(2):203. doi: 10.3390/v16020203. Viruses. 2024. PMID: 38399979 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
