

Bilirubin as an indicator of cardiometabolic health: a cross-sectional analysis in the UK Biobank
- PMID: 35436955
- PMCID: PMC9017025
- DOI: 10.1186/s12933-022-01484-x
Bilirubin as an indicator of cardiometabolic health: a cross-sectional analysis in the UK Biobank
Abstract
Background: Mildly elevated bilirubin, a by-product of hemoglobin breakdown, might mitigate cardiometabolic risk factors including adiposity, dyslipidemia, and high blood pressure (BP). We investigated the cross-sectional relationship between (total) bilirubin and baseline cardiometabolic risk factors in 467,519 UK Biobank study participants.
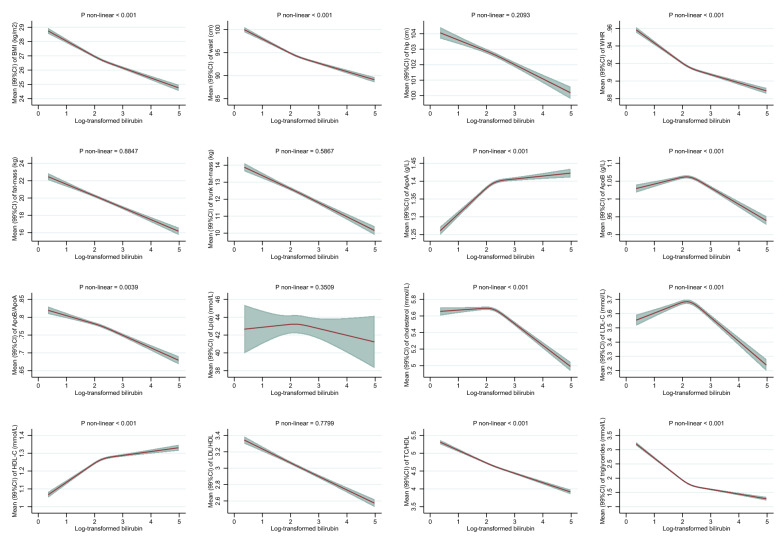
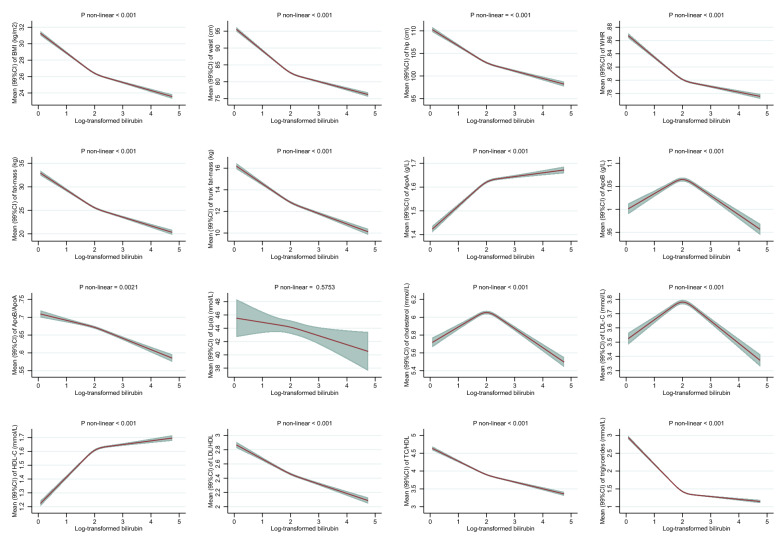
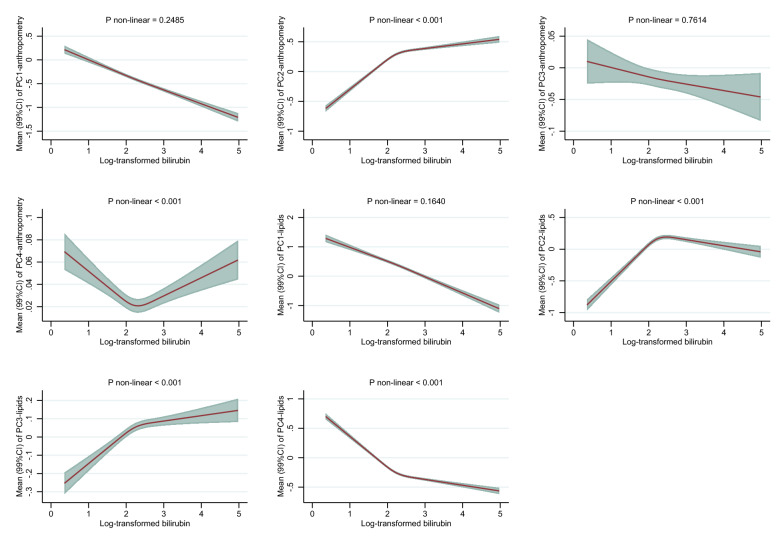
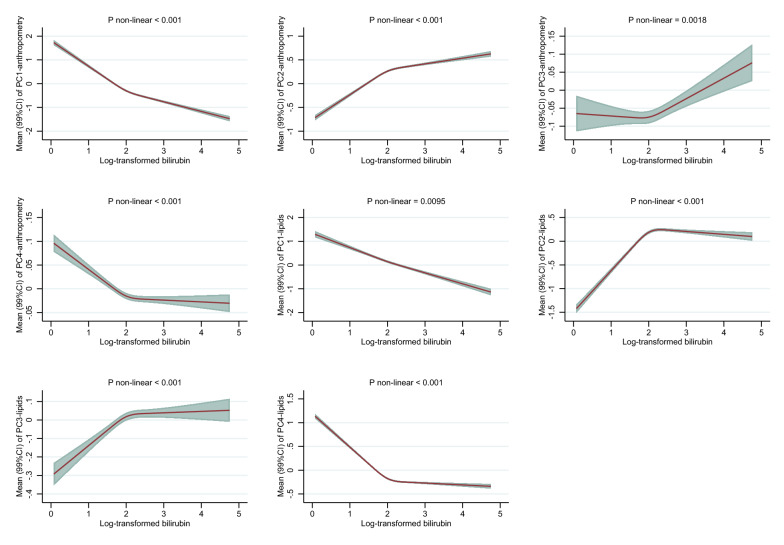
Methods: We used multivariable-adjusted linear regression to estimate associations between bilirubin levels and risk factors of cardiometabolic diseases including body mass index (BMI), waist and hip circumferences (WC, HC), waist-to-hip ratio (WHR), fat mass (FM), and trunk FM, and the blood lipids: apolipoprotein A-I (apoA-I), apolipoprotein B (apoB), apoB/apoA-I, lipoprotein (a), total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), LDL/HDL, TC/HDL, triglycerides (TG). Log-transformed bilirubin was modelled with restricted cubic splines and predicted mean values with 99% confidence intervals (CI) for each risk marker were estimated, separately. Second, we applied principal component analysis (PCA) for dimension reduction to in turn six anthropometric traits (height, weight, BMI, WC, HC, and WHR) and all above lipids. Last, we estimated associations (99%CI) between bilirubin and three components of the metabolic syndrome, i.e. WC, TG, and BP using logistic regression.
Results: After multivariable adjustments, higher levels of bilirubin were inversely associated with indicators of general adiposity (BMI and FM) and of body fat distribution (WC, HC, WHR, and trunk FM) in both men and women. For example, women with mildly elevated bilirubin (95th percentile equal to 15.0 µmol/L), compared to women with low bilirubin (5th percentile equal to 4.5 µmol/L), had on average a 2.0 kg/m2 (99% CI 1.9-2.1) lower BMI. Inverse associations were also observed with dyslipidemia among men and women. For example, mildly elevated bilirubin among men (95th percentile equal to 19.4 µmol/L) compared to low levels of bilirubin (5th percentile equal to 5.5 µmol/L) were associated with approx. 0.55 mmol/L (99% CI 0.53-0.56) lower TG levels, with similar inverse associations among women. Multiple-trait analyses using PCA confirmed single-trait analyses. Men and women with mildly elevated bilirubin levels ≥ 17.1 µmol/L, compared to low-normal bilirubin < 10 µmol/L had 13% (99% CI 8%-18%) and 11% (99% CI 4%-17%) lower odds of exceeding systolic BP levels of ≥ 130 mm Hg, respectively.
Conclusions: Higher levels of bilirubin were inversely associated with cardiometabolic risk factors including adiposity, dyslipidemia, and hypertension.
Keywords: Bilirubin; Metabolic syndrome; Obesity; UK Biobank.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Excess accumulation of body fat is related to dyslipidemia in normal-weight subjects.Int J Obes Relat Metab Disord. 2004 Feb;28(2):242-7. doi: 10.1038/sj.ijo.0802528. Int J Obes Relat Metab Disord. 2004. PMID: 14610531
-
Prevalence of dyslipidemia and associated risk factors among Turkish adults: Trabzon lipid study.Endocrine. 2008 Aug-Dec;34(1-3):36-51. doi: 10.1007/s12020-008-9100-z. Epub 2008 Nov 12. Endocrine. 2008. PMID: 19003544
-
A comparative research on obesity hypertension by the comparisons and associations between waist circumference, body mass index with systolic and diastolic blood pressure, and the clinical laboratory data between four special Chinese adult groups.Clin Exp Hypertens. 2018;40(1):16-21. doi: 10.1080/10641963.2017.1281940. Epub 2017 Oct 30. Clin Exp Hypertens. 2018. PMID: 29083240
-
Association between elevated serum alanine aminotransferase and cardiometabolic risk factors in rural Chinese population: a cross-sectional study.BMC Cardiovasc Disord. 2015 Jul 10;15:65. doi: 10.1186/s12872-015-0060-y. BMC Cardiovasc Disord. 2015. PMID: 26160405 Free PMC article.
-
The association of maternal gestational weight gain with cardiometabolic risk factors in offspring: a systematic review and meta-analysis.Nutr Rev. 2025 Feb 1;83(2):e106-e115. doi: 10.1093/nutrit/nuae027. Nutr Rev. 2025. PMID: 38607346
Cited by
-
The Association between Serum Lipid Profile Levels and Hypertension Grades: A Cross-Sectional Study at a Health Examination Center.High Blood Press Cardiovasc Prev. 2025 Jan;32(1):87-98. doi: 10.1007/s40292-024-00683-9. Epub 2024 Nov 27. High Blood Press Cardiovasc Prev. 2025. PMID: 39602007
-
Development and validation of a new prediction model for calcific aortic valve stenosis.J Thorac Dis. 2022 Oct;14(10):4044-4054. doi: 10.21037/jtd-22-1157. J Thorac Dis. 2022. PMID: 36389293 Free PMC article.
-
Association between bilirubin and biomarkers of metabolic health and oxidative stress in the MARK-AGE cohort.iScience. 2024 Jun 9;27(7):110234. doi: 10.1016/j.isci.2024.110234. eCollection 2024 Jul 19. iScience. 2024. PMID: 39021797 Free PMC article.
-
Mildly elevated serum bilirubin and its correlations with lipid levels among male patients undergoing health checkups.Lipids Health Dis. 2023 Dec 4;22(1):213. doi: 10.1186/s12944-023-01979-w. Lipids Health Dis. 2023. PMID: 38049818 Free PMC article.
-
The associations of psychopathology and metabolic parameters with serum bilirubin levels in patients with acute-episode and drug-free schizophrenia: a 5-year retrospective study using an electronic medical record system.BMC Psychiatry. 2024 May 29;24(1):403. doi: 10.1186/s12888-024-05862-5. BMC Psychiatry. 2024. PMID: 38811905 Free PMC article.
References
-
- Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet (London, England). 2016;388(10053):1659–724. - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
