

Identifying molecular mediators of the relationship between body mass index and endometrial cancer risk: a Mendelian randomization analysis
- PMID: 35436960
- PMCID: PMC9017004
- DOI: 10.1186/s12916-022-02322-3
Identifying molecular mediators of the relationship between body mass index and endometrial cancer risk: a Mendelian randomization analysis
Abstract
Background: Endometrial cancer is the most common gynaecological cancer in high-income countries. Elevated body mass index (BMI) is an established modifiable risk factor for this condition and is estimated to confer a larger effect on endometrial cancer risk than any other cancer site. However, the molecular mechanisms underpinning this association remain unclear. We used Mendelian randomization (MR) to evaluate the causal role of 14 molecular risk factors (hormonal, metabolic and inflammatory markers) in endometrial cancer risk. We then evaluated and quantified the potential mediating role of these molecular traits in the relationship between BMI and endometrial cancer using multivariable MR.
Methods: Genetic instruments to proxy 14 molecular risk factors and BMI were constructed by identifying single-nucleotide polymorphisms (SNPs) reliably associated (P < 5.0 × 10-8) with each respective risk factor in previous genome-wide association studies (GWAS). Summary statistics for the association of these SNPs with overall and subtype-specific endometrial cancer risk (12,906 cases and 108,979 controls) were obtained from a GWAS meta-analysis of the Endometrial Cancer Association Consortium (ECAC), Epidemiology of Endometrial Cancer Consortium (E2C2) and UK Biobank. SNPs were combined into multi-allelic models and odds ratios (ORs) and 95% confidence intervals (95% CIs) were generated using inverse-variance weighted random-effects models. The mediating roles of the molecular risk factors in the relationship between BMI and endometrial cancer were then estimated using multivariable MR.
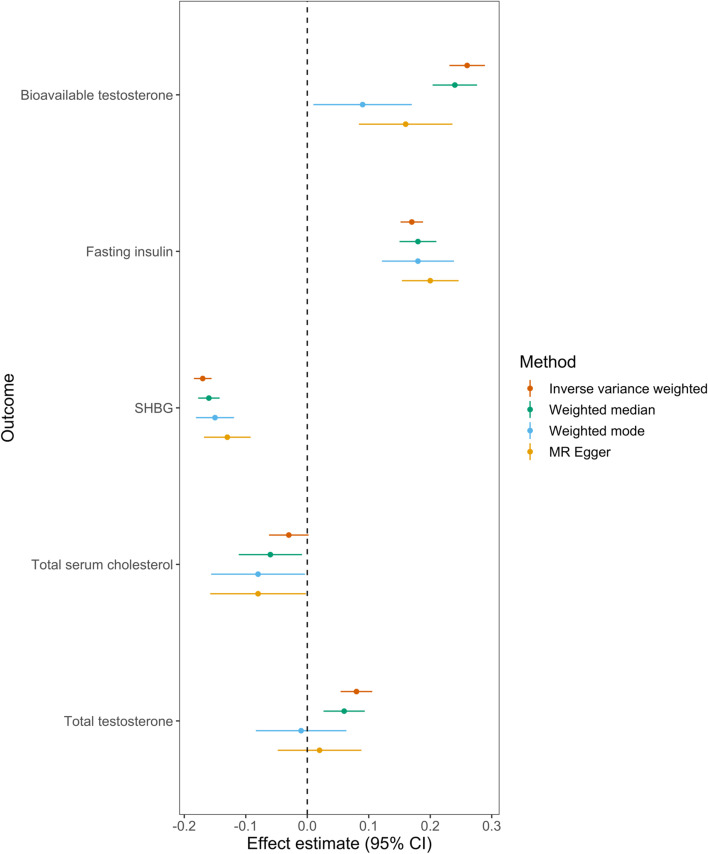
Results: In MR analyses, there was strong evidence that BMI (OR per standard deviation (SD) increase 1.88, 95% CI 1.69 to 2.09, P = 3.87 × 10-31), total testosterone (OR per inverse-normal transformed nmol/L increase 1.64, 95% CI 1.43 to 1.88, P = 1.71 × 10-12), bioavailable testosterone (OR per natural log transformed nmol/L increase: 1.46, 95% CI 1.29 to 1.65, P = 3.48 × 10-9), fasting insulin (OR per natural log transformed pmol/L increase: 3.93, 95% CI 2.29 to 6.74, P = 7.18 × 10-7) and sex hormone-binding globulin (SHBG, OR per inverse-normal transformed nmol/L increase 0.71, 95% CI 0.59 to 0.85, P = 2.07 × 10-4) had a causal effect on endometrial cancer risk. Additionally, there was suggestive evidence that total serum cholesterol (OR per mg/dL increase 0.90, 95% CI 0.81 to 1.00, P = 4.01 × 10-2) had an effect on endometrial cancer risk. In mediation analysis, we found evidence for a mediating role of fasting insulin (19% total effect mediated, 95% CI 5 to 34%, P = 9.17 × 10-3), bioavailable testosterone (15% mediated, 95% CI 10 to 20%, P = 1.43 × 10-8) and SHBG (7% mediated, 95% CI 1 to 12%, P = 1.81 × 10-2) in the relationship between BMI and endometrial cancer risk.
Conclusions: Our comprehensive MR analysis provides insight into potential causal mechanisms linking BMI with endometrial cancer risk and suggests targeting of insulinemic and hormonal traits as a potential strategy for the prevention of endometrial cancer.
Keywords: Bioavailable testosterone; Body mass index; Endometrial cancer; Fasting insulin; Mendelian randomization; Sex hormone-binding globulin.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures





References
-
- Howlader NNA, Krapcho M, Miller D, Bishop K, Kosary CL, Yu M, et al., editors. SEER Cancer Statistics Review, 1975-2014, National Cancer Institute. Bethesda, https://seer.cancer.gov/archive/csr/1975_2014/. Based on November 2016 SEER data submission, posted to the SEER web site; 2017.
Publication types
MeSH terms
Substances
Grants and funding
- R01 CA134958/CA/NCI NIH HHS/United States
- MC_QA137853/MRC_/Medical Research Council/United Kingdom
- R01 CA058598/CA/NCI NIH HHS/United States
- MC_UU_00011/1/MRC_/Medical Research Council/United Kingdom
- MR/T002239/1/MRC_/Medical Research Council/United Kingdom
- MC_UU_00011/6/MRC_/Medical Research Council/United Kingdom
- U19 CA148112/CA/NCI NIH HHS/United States
- MC_PC_17228/MRC_/Medical Research Council/United Kingdom
- 001/WHO_/World Health Organization/International
- R01 CA149429/CA/NCI NIH HHS/United States
- MC_UU_00011/4/MRC_/Medical Research Council/United Kingdom
- U19 CA148065/CA/NCI NIH HHS/United States
- WT_/Wellcome Trust/United Kingdom
LinkOut - more resources
Full Text Sources
Miscellaneous
