

Non-glandular findings on breast ultrasound. Part I: a pictorial review of superficial lesions
- PMID: 35438461
- PMCID: PMC9705641
- DOI: 10.1007/s40477-021-00619-2
Non-glandular findings on breast ultrasound. Part I: a pictorial review of superficial lesions
Abstract
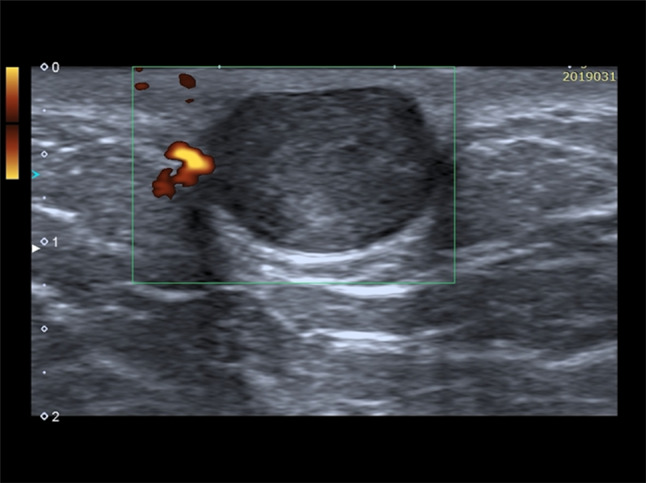
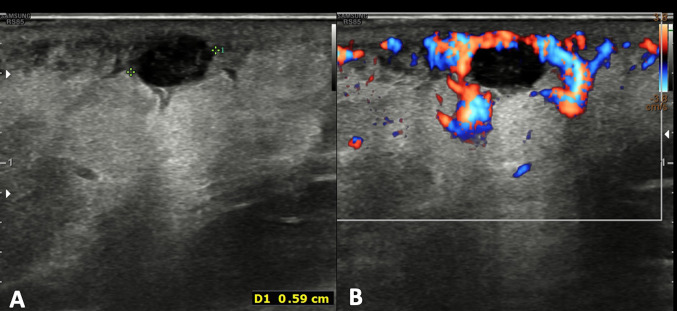
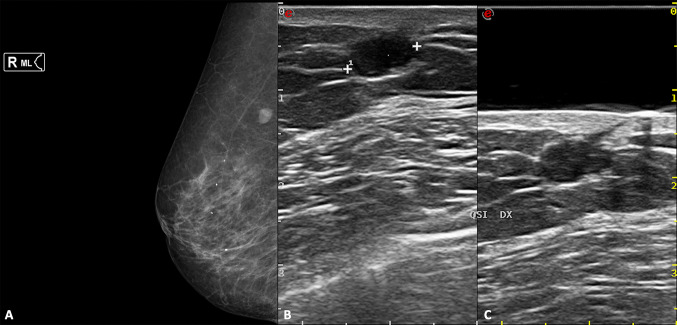
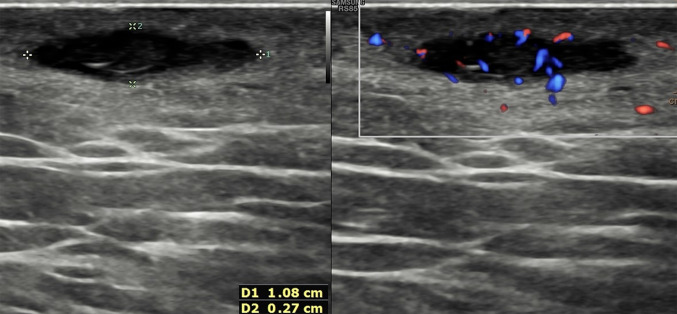
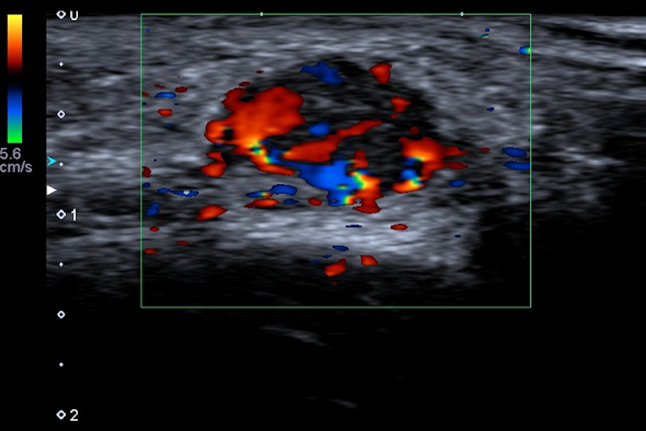
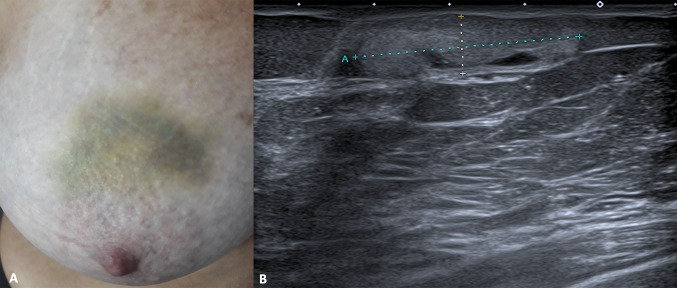
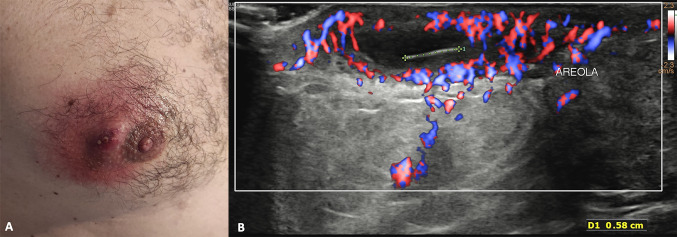
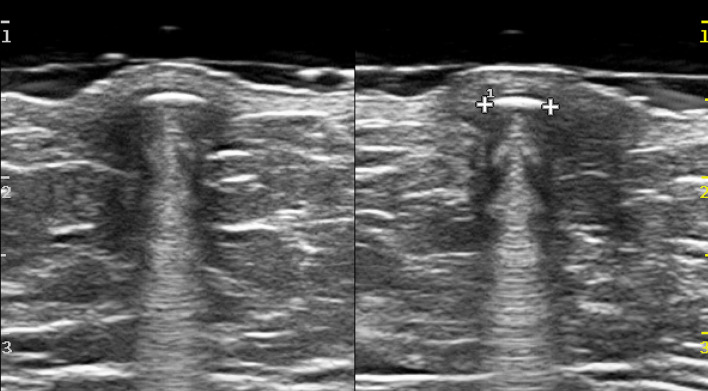
Ultrasound (US) represents the first-level imaging technique in the assessment of breast in young patients, whereas it is complementary to mammography in adult ones. It is not uncommon to encounter non-glandular mass during either screening or diagnostic breast US; sometimes the evaluation of palpable lump may be the reason of clinician's US request. The breast US field-of-view includes not only the glandular parenchyma, but also the tissues located anterior and posterior to it, from the skin to the ribs. In this setting, the radiologist must be familiar with the non-glandular breast diseases, which can occur in the superficial layers as well as in the chest wall. The differential diagnosis varies according to anatomic layer, so the anatomic origin is the first feature to assess and the correct localization is needed to avoid misdiagnosis and to choose, when requested, the second diagnostic step, imaging or histologic analysis. This paper is the first of two focused on non-glandular breast lesions; characterization, differential diagnosis, and pitfalls of superficial lesions are reviewed. They may be located in the dermis or hypodermis: the former are usually benign skin lesions, whereas the latter, although usually benign, may arise also from the anterior terminal lobular units, hence the papilloma, fibroadenomas, and breast cancers should be included in the differential diagnosis. US is more sensitive than CT and MRI in the assessment of superficial lesions due to higher spatial resolution.
Keywords: Breast Ultrasound; Characterization; Differential Diagnosis; Hypodermal Lesions; Pitfalls; Skin Lesions; Superficial non-glandular Lesions.
© 2022. Società Italiana di Ultrasonologia in Medicina e Biologia (SIUMB).
Conflict of interest statement
We confirm that this work is original and has not been published elsewhere nor is it currently under consideration for publication elsewhere. Publication is approved by all authors and by the responsible authorities where the work was carried out. Each author have participated sufficiently in any submission to take public responsibility for its content. The authors have no conflicts of interest. Written informed consent was obtained from all patients, and the study was approved by the ethics committee of the institution.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
