

Evaluation of multinodular goiter and primary hyperparathyroidism leads to a diagnosis of AL amyloidosis
- PMID: 35440089
- PMCID: PMC9019962
- DOI: 10.1186/s13044-022-00125-5
Evaluation of multinodular goiter and primary hyperparathyroidism leads to a diagnosis of AL amyloidosis
Abstract
Background: Amyloid goiter, defined as excess amyloid within the thyroid gland in such quantities that it produces a clinically apparent goiter, is a very rare manifestation of systemic amyloidosis with cases commonly seen in the setting of Amyloid A (AA) amyloidosis. Amyloid goiter as the primary clinical manifestation secondary to Amyloid light chain (AL) amyloidosis is very rare. We present a case of AL amyloidosis with initial manifestation as goiter with amyloid deposition in the thyroid and the parathyroid gland.
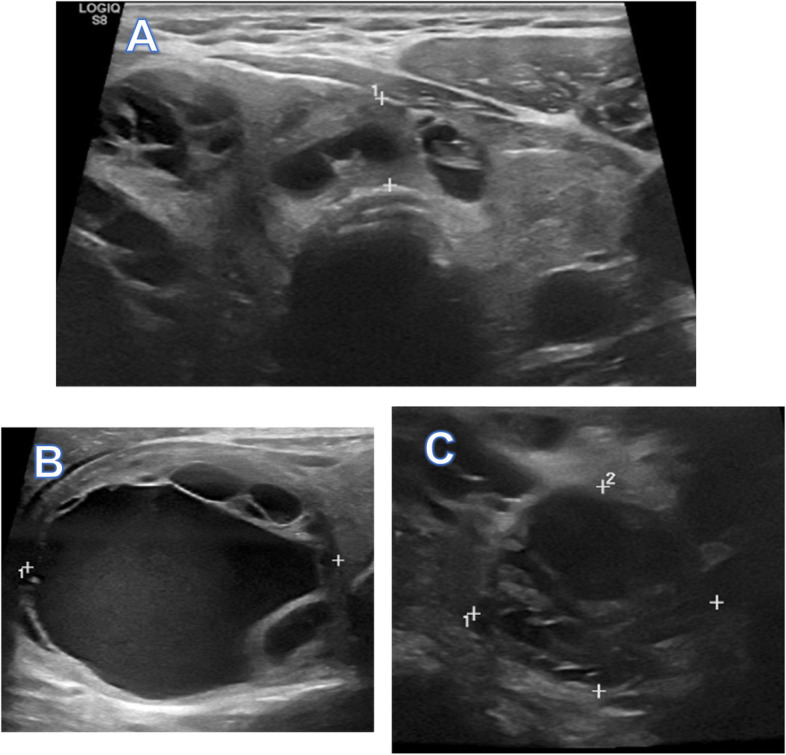
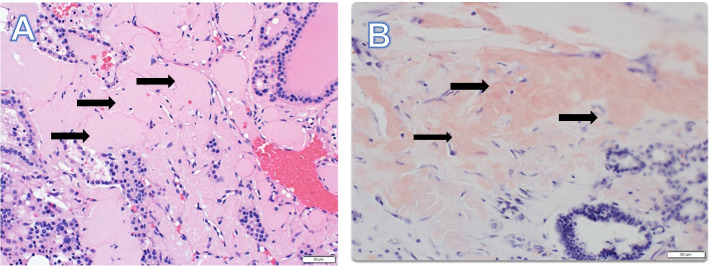
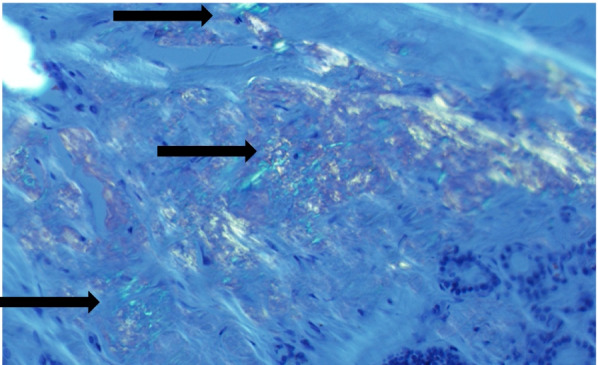
Case presentation: A 73 year old male presented with goiter and compressive symptoms of dysphagia and hoarseness. Laboratory workup revealed normal thyroid function, nephrotic range proteinuria, elevated serum calcium level with an elevated parathyroid hormone level (PTH) consistent with primary hyperparathyroidism. Thyroid ultrasound showed an asymmetric goiter with three dominant nodules. Cervical computed tomography revealed a goiter with substernal extension and deviation of the trachea. Fine needle aspiration was unsatisfactory. There was also evidence of osteoporosis and hypercalciuria with negative Sestamibi scan for parathyroid adenoma. The patient underwent a total thyroidectomy and one gland parathyroidectomy. Pathology revealed benign thyroid parenchyma with diffuse amyloid deposition in the thyroid and parathyroid gland that stained apple green birefringence under polarized light on Congo Red stain. Immunochemical staining detected AL amyloid deposition of the lambda type. Bone marrow biopsy revealed an excess monoclonal lambda light chain of plasma cells consistent with a diagnosis of AL amyloidosis secondary to multiple myeloma affecting the kidney, thyroid, parathyroid gland, and heart. He was treated with 4 cycles of chemotherapy with a decrease in the M spike and light chains with a plan to pursue a bone marrow transplant.
Conclusion: Amyloid goiter as the primary clinical manifestation secondary to AL amyloidosis with deposition in the thyroid and parathyroid gland is rare. The top differential for amyloid deposits in the thyroid includes systemic amyloidosis or medullary thyroid carcinoma. The definitive diagnosis lies in the histopathology of the thyroid tissue. To diagnose systemic amyloidosis as the etiology for a goiter, a solid understanding of the causes of systemic amyloidosis coupled with a thorough evaluation of the patient's history and laboratory data is necessary.
Keywords: AL amyloidosis; Amyloid; Amyloid goiter; Amyloid light chain.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Nodular goiter with amyloid deposition in an elderly patient: fine-needle cytology diagnosis and review of the literature.BMC Surg. 2013;13 Suppl 2(Suppl 2):S43. doi: 10.1186/1471-2482-13-S2-S43. Epub 2013 Oct 8. BMC Surg. 2013. PMID: 24267036 Free PMC article. Review.
-
Co-occurrence of Amyloid Goiter and Adipose Metaplasia in a Patient With History of Pulmonary Tuberculosis: A Case Report.Cureus. 2023 Mar 11;15(3):e36008. doi: 10.7759/cureus.36008. eCollection 2023 Mar. Cureus. 2023. PMID: 37041909 Free PMC article.
-
Amyloid goiter as a manifestation of primary systemic amyloidosis.Thyroid. 2007 Jan;17(1):77-80. doi: 10.1089/thy.2006.0045. Thyroid. 2007. PMID: 17274755
-
AMYLOID GOITER AS THE FIRST RECOGNIZABLE MANIFESTATION OF IMMUNOGLOBULIN LIGHT CHAIN AMYLOIDOSIS.AACE Clin Case Rep. 2019 Jun 26;5(5):e326-e329. doi: 10.4158/ACCR-2019-0161. eCollection 2019 Sep-Oct. AACE Clin Case Rep. 2019. PMID: 31967063 Free PMC article.
-
Al amyloidosis.Orphanet J Rare Dis. 2012 Aug 21;7:54. doi: 10.1186/1750-1172-7-54. Orphanet J Rare Dis. 2012. PMID: 22909024 Free PMC article. Review.
Cited by
-
Amyloid Goiter, Papillary Thyroid Carcinoma, and Diffuse Thyroid Lipomatosis: A Case Report of a Rare Association.Cureus. 2024 Oct 11;16(10):e71245. doi: 10.7759/cureus.71245. eCollection 2024 Oct. Cureus. 2024. PMID: 39525182 Free PMC article.
-
Amyloid Goiter Secondary to Behcet's Disease: A Case Report and Literature Review.Cureus. 2023 Nov 29;15(11):e49650. doi: 10.7759/cureus.49650. eCollection 2023 Nov. Cureus. 2023. PMID: 38161812 Free PMC article.
References
LinkOut - more resources
Full Text Sources
