

Impact of Previous Stroke on Clinical Outcome in Elderly Patients With Nonvalvular Atrial Fibrillation: ANAFIE Registry
- PMID: 35440169
- PMCID: PMC9311295
- DOI: 10.1161/STROKEAHA.121.038285
Impact of Previous Stroke on Clinical Outcome in Elderly Patients With Nonvalvular Atrial Fibrillation: ANAFIE Registry
Abstract
Background: We determined the long-term event incidence among elderly patients with nonvalvular atrial fibrillation in terms of history of stroke/transient ischemic attack (TIA) and oral anticoagulation.
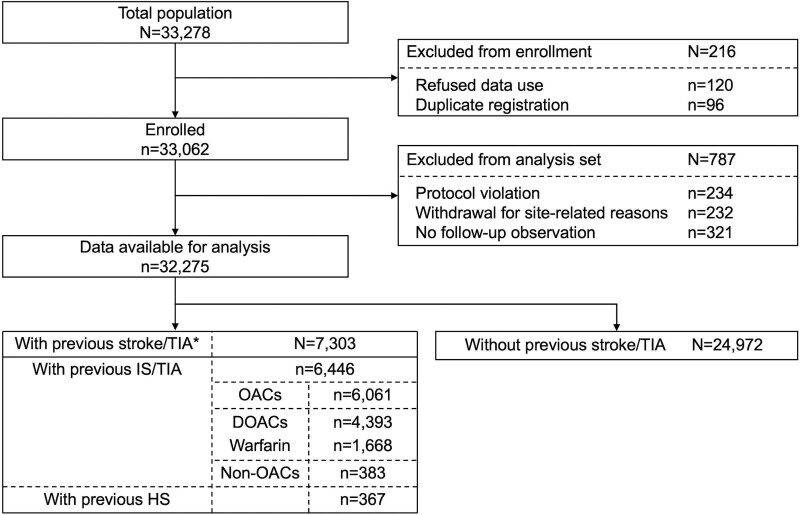
Methods: Patients aged ≥75 years with documented nonvalvular atrial fibrillation enrolled in the prospective, multicenter, observational All Nippon Atrial Fibrillation in the Elderly Registry between October 2016 and January 2018 were divided into 2 groups according to history of stroke/TIA. The primary end point was the occurrence of stroke/systemic embolism within 2 years, and secondary end points were major bleeding and all-cause death within 2 years. Cox models were used to determine whether there was a difference in the hazard of each end point in patients with/without history of stroke/TIA, and in ischemic stroke/TIA survivors taking direct oral anticoagulants versus those taking warfarin.
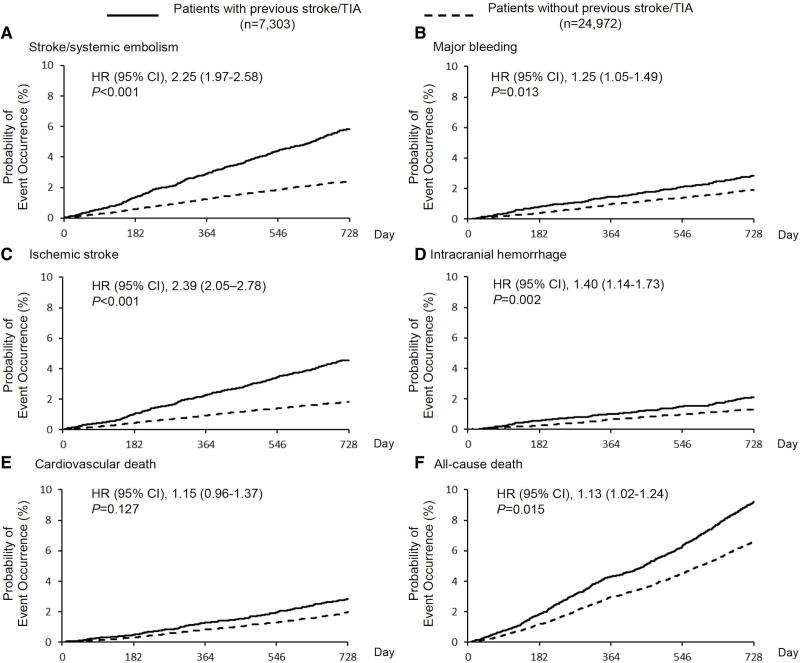
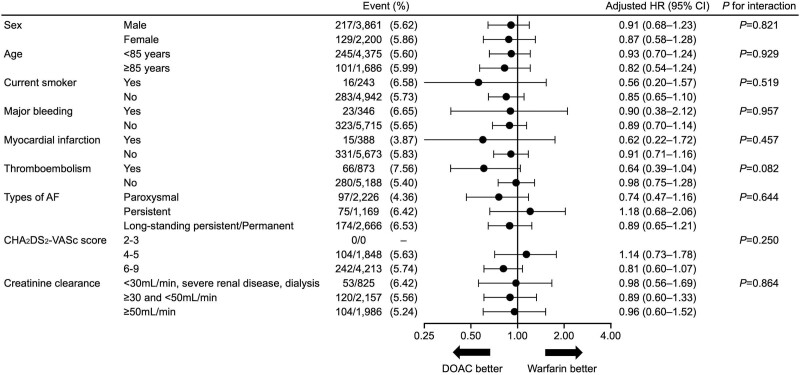
Results: Of 32 275 evaluable patients (13 793 women [42.7%]; median age, 81.0 years), 7304 (22.6%) had a history of stroke/TIA. The patients with previous stroke/TIA were more likely to be male and older and had higher hazard rates of stroke/systemic embolism (adjusted hazard ratio, 2.25 [95% CI, 1.97-2.58]), major bleeding (1.25, 1.05-1.49), and all-cause death (1.13, 1.02-1.24) than the other groups. Of 6446 patients with prior ischemic stroke/TIA, 4393 (68.2%) were taking direct oral anticoagulants and 1668 (25.9%) were taking warfarin at enrollment. The risk of stroke/systemic embolism was comparable between these 2 groups (adjusted hazard ratio, 0.90 [95% CI, 0.71-1.14]), while the risk of major bleeding (0.67, 0.48-0.94), intracranial hemorrhage (0.57, 0.39-0.85), and cardiovascular death (0.71, 0.51-0.99) was lower among those taking direct oral anticoagulants.
Conclusions: Patients aged ≥75 years with nonvalvular atrial fibrillation and previous stroke/TIA more commonly had subsequent ischemic and hemorrhagic events than those without previous stroke/TIA. Among patients with previous ischemic stroke/TIA, the risk of hemorrhagic events was lower in patients taking direct oral anticoagulants compared with warfarin.
Registration: URL: https://www.
Clinicaltrials: gov; Unique Identifier: UMIN000024006.
Keywords: atrial fibrillation; cardioembolism; direct oral anticoagulants; elderly; intracranial hemorrhage; stroke.
Figures
References
-
- Kannel WB, Wolf PA, Benjamin EJ, Levy D. Prevalence, incidence, prognosis, and predisposing conditions for atrial fibrillation: population-based estimates. Am J Cardiol. 1998;82(8A):2N–9N. doi: 10.1016/s0002-9149(98)00583-9 - PubMed
-
- Schnabel RB, Yin X, Gona P, Larson MG, Beiser AS, McManus DD, Newton-Cheh C, Lubitz SA, Magnani JW, Ellinor PT, et al. 50 year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: a cohort study. Lancet. 2015;386:154–162. doi: 10.1016/S0140-6736(14)61774-8 - PMC - PubMed
-
- McGrath ER, Kapral MK, Fang J, Eikelboom JW, Conghaile A, O’Conghaile A, Canavan M, O’Donnell MJ; Investigators of the Ontario Stroke Registry. Association of atrial fibrillation with mortality and disability after ischemic stroke. Neurology. 2013;81:825–832. doi: 10.1212/WNL.0b013e3182a2cc15 - PubMed
-
- Diener HC, Connolly SJ, Ezekowitz MD, Wallentin L, Reilly PA, Yang S, Xavier D, Di Pasquale G, Yusuf S; RE-LY Study Group. Dabigatran compared with warfarin in patients with atrial fibrillation and previous transient ischaemic attack or stroke: a subgroup analysis of the RE-LY trial. Lancet Neurol. 2010;9:1157–1163. doi: 10.1016/S1474-4422(10)70274-X - PubMed
-
- Hankey GJ, Patel MR, Stevens SR, Becker RC, Breithardt G, Carolei A, Diener HC, Donnan GA, Halperin JL, Mahaffey KW, et al. ; ROCKET AF Steering Committee Investigators. Rivaroxaban compared with warfarin in patients with atrial fibrillation and previous stroke or transient ischaemic attack: a subgroup analysis of ROCKET AF. Lancet Neurol. 2012;11:315–322. doi: 10.1016/S1474-4422(12)70042-X - PubMed
Publication types
MeSH terms
Substances
Associated data
- Actions
LinkOut - more resources
Full Text Sources
Medical
