

Cardio-onco-metabolism: metabolic remodelling in cardiovascular disease and cancer
- PMID: 35440740
- PMCID: PMC10112835
- DOI: 10.1038/s41569-022-00698-6
Cardio-onco-metabolism: metabolic remodelling in cardiovascular disease and cancer
Abstract
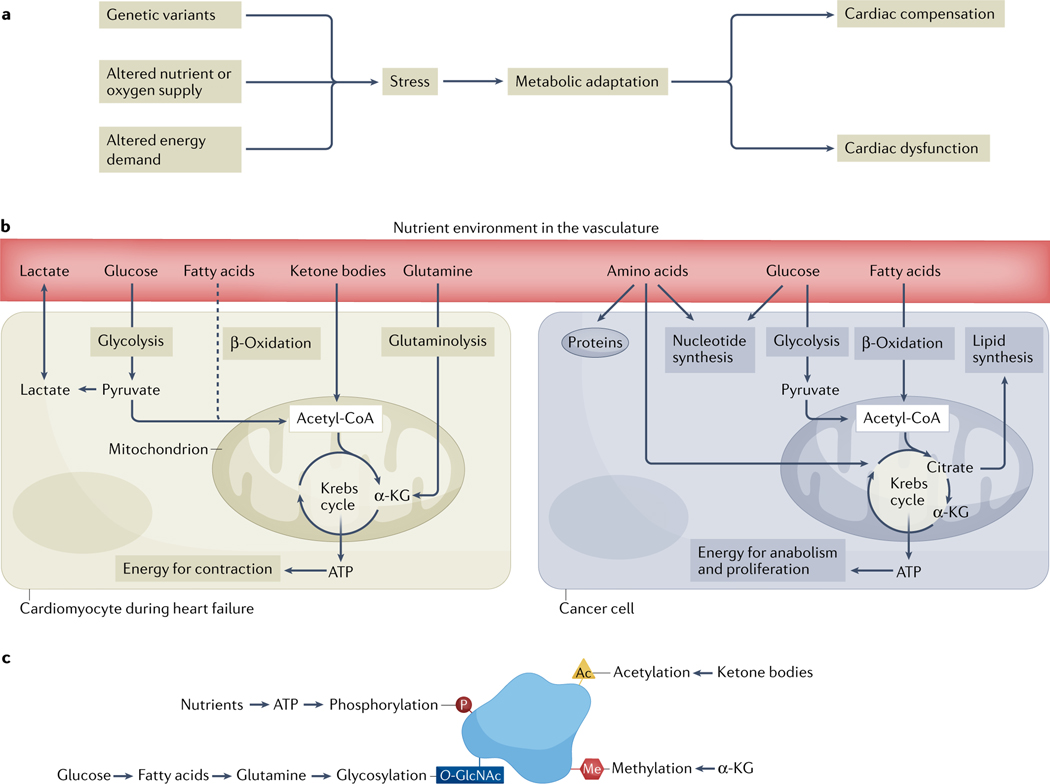
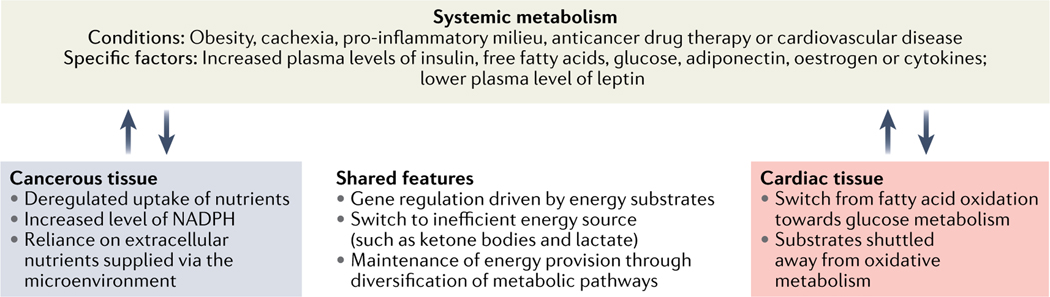
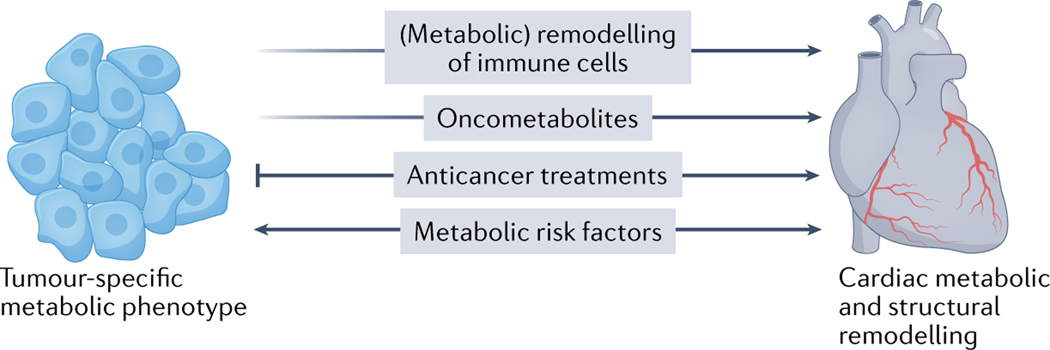
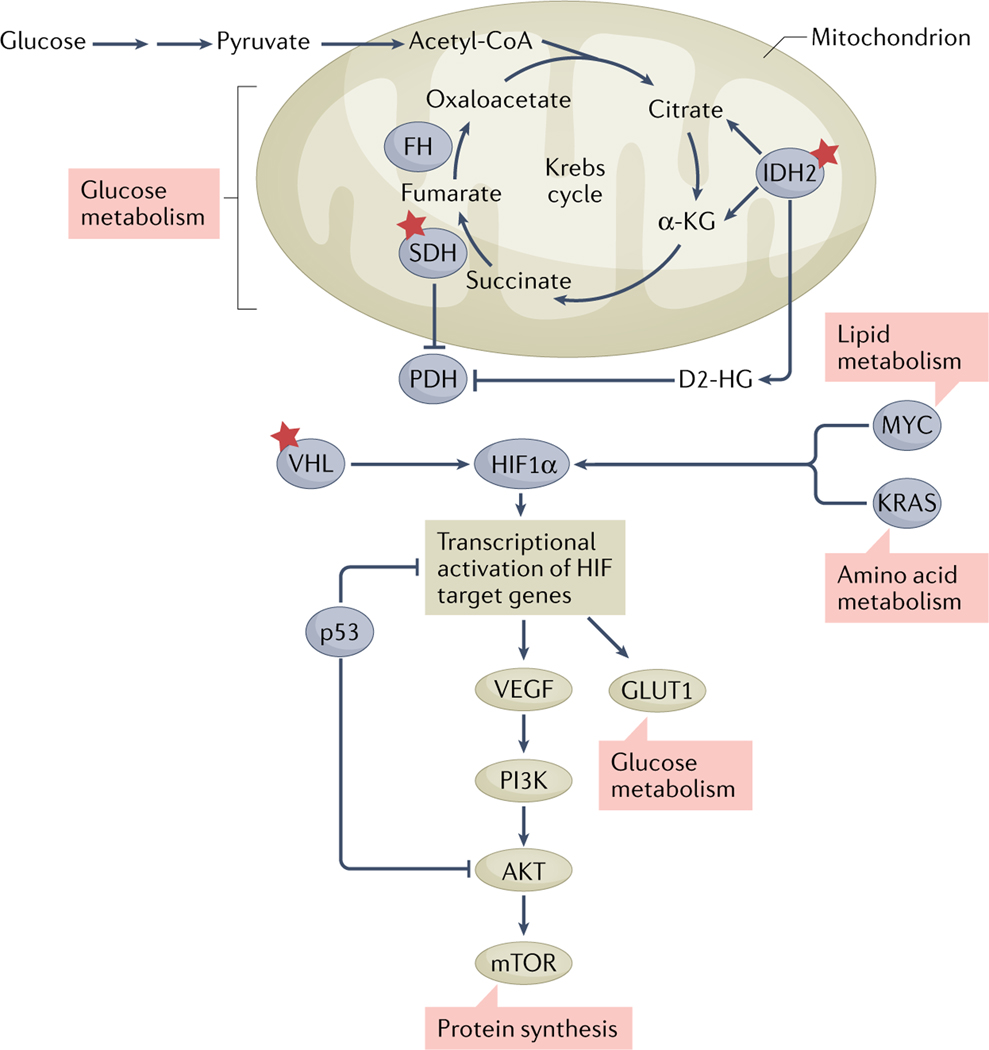
Cardiovascular disease and cancer are the two leading causes of morbidity and mortality in the world. The emerging field of cardio-oncology has revealed that these seemingly disparate disease processes are intertwined, owing to the cardiovascular sequelae of anticancer therapies, shared risk factors that predispose individuals to both cardiovascular disease and cancer, as well the possible potentiation of cancer growth by cardiac dysfunction. As a result, interest has increased in understanding the fundamental biological mechanisms that are central to the relationship between cardiovascular disease and cancer. Metabolism, appropriate regulation of energy, energy substrate utilization, and macromolecular synthesis and breakdown are fundamental processes for cellular and organismal survival. In this Review, we explore the emerging data identifying metabolic dysregulation as an important theme in cardio-oncology. We discuss the growing recognition of metabolic reprogramming in cardiovascular disease and cancer and view the novel area of cardio-oncology through the lens of metabolism.
© 2022. Springer Nature Limited.
Conflict of interest statement
Competing interests
A.K. declares no competing interests.
Figures
References
-
- Moslehi JJ Cardiovascular toxic effects of targeted cancer therapies. N. Engl. J. Med 375, 1457–1467 (2016). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
