

A multicenter study of the 5-year trends in robot-assisted spine surgery outcomes and complications
- PMID: 35441099
- PMCID: PMC8990386
- DOI: 10.21037/jss-21-102
A multicenter study of the 5-year trends in robot-assisted spine surgery outcomes and complications
Abstract
Background: Although a growing amount of literature that suggests robots are safe and can achieve comparable outcomes to conventional techniques, much of this literature is limited by small sample sizes and single-surgeon or single center series. Furthermore, it is unclear what the impact of robotic technology has made on operative and clinical outcomes over time. This is the first and largest multicenter study to examine the trends in outcomes and complications after robot-assisted spine surgery over a 5-year period.
Methods: Adult (≥18 years old) patients who underwent spine surgery with robot-assistance between 2015 and 2019 at four unique spine centers. The robotic systems used included the Mazor Renaissance, Mazor X, and Mazor Stealth Edition. Patients with incomplete data were excluded from this study. The minimum follow-up was 90 days.
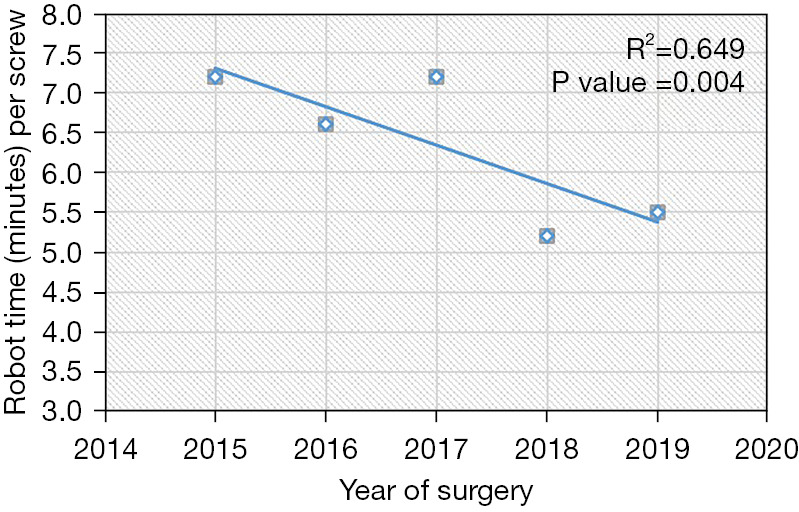
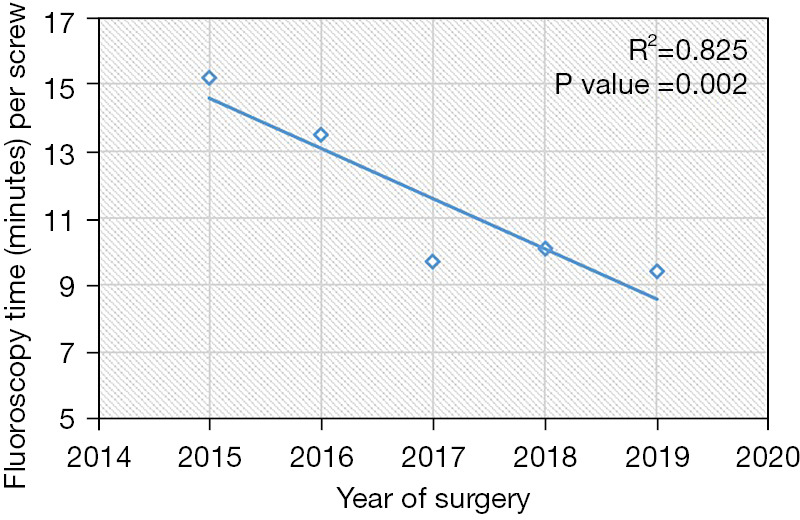
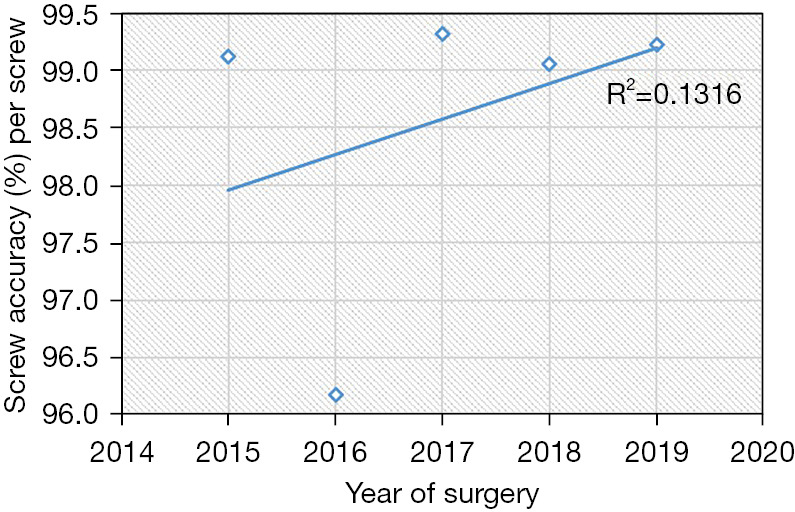
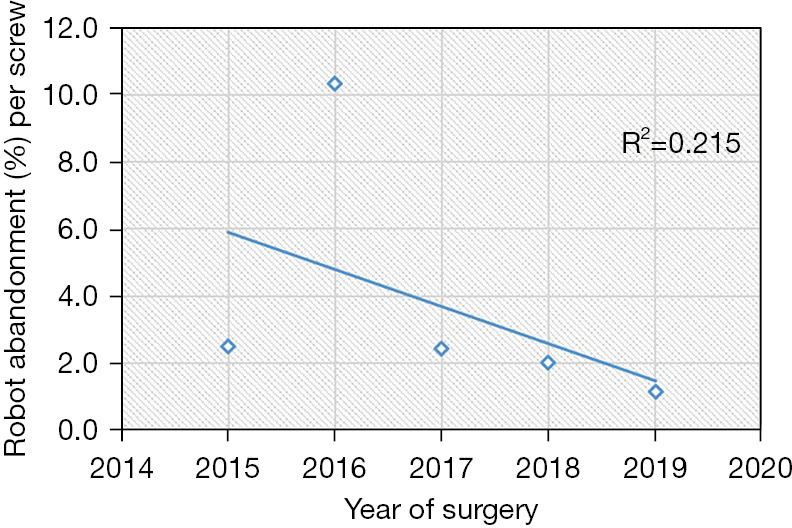
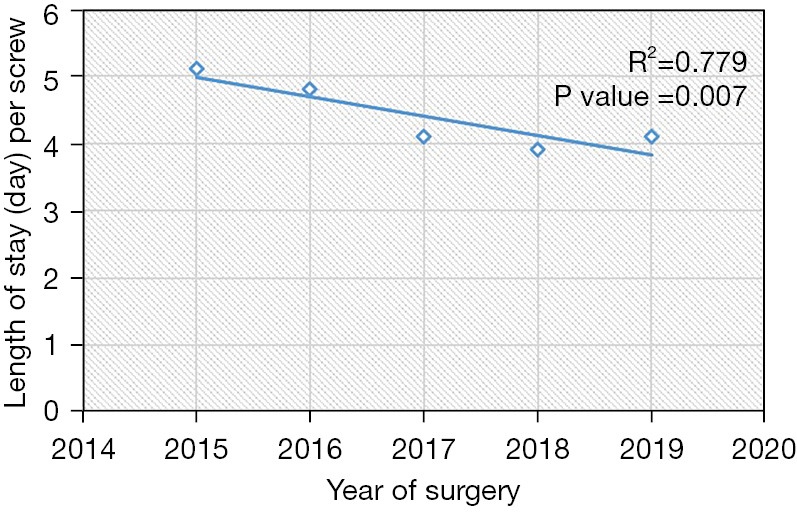
Results: A total of 722 adult patients were included (117 Renaissance, 477 X, 128 Stealth). Most patient and operative factors (e.g., sex, tobacco status, total instrumented levels, and pelvic fixation,) were similar across the years. Mean ± standard deviation Charlson comorbidity index (CCI) was 1.5±1.5. The most commonly reported diagnoses included high grade spondylolisthesis (40.6%), degenerative disc disease (18.4%), and degenerative scoliosis (17.6%). Mean (standard deviation) number of instrumented levels was 3.8±3.4. From 2015 to 2019, average robot time per screw improved from 7.2 to 5.5 minutes (P=0.004, R2=0.649). Average fluoroscopy time per screw improved from 15.2 to 9.4 seconds (P=0.002). Rates of both intraoperative screw exchange for misplaced screw (2015-2016: 2.7%, 2019: 0.8%, P=0.0115, R2=0.1316) and robot abandonment (2015-2016: 7.1%, 2019: 1.1%, P=0.011, R2=0.215) improved significantly over time. The incidence of other intraoperative complications (e.g., dural tear, loss of motor/sensory function, blood transfusion) remained consistently low, but similar throughout the years. The length of stay (LOS) decreased by nearly 1 day from 2015 to 2019 (P=0.007, R2=0.779). 90-day reoperation rates did not change significantly.
Conclusions: At four institutions among seven surgeons, we demonstrate robot screw accuracy, reliability, operative efficiency, and radiation exposure improved significantly from 2015 to 2019. 90-day complication rates remained low and LOS decreased significantly with time. These findings further validate continued usage of robot-assisted spine surgery and the path toward improved value-based care.
Keywords: Robot-assisted spine surgery; pedicle screw; robot abandonment; short-term complications.
2022 Journal of Spine Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jss.amegroups.com/article/view/10.21037/jss-21-102/coif). SZ serves as an unpaid editorial board member of Journal of Spine Surgery. EJ reports consulting fees from Stryker, Medtronic, and Innovasis outside the submitted work. CH reports personal fees from Medtronic, Globus Medical, Spineart, and Innovasis outside the submitted work. CRG reports royalties from Stryker/K2M and Medtronic; consulting fees from Stryker/K2M, Medtronic; educational grant support from Medtronic, is on an advisory board for Stryker/K2M, Medtronic, and Augmedics, and owns stock in Augmedics and NSite. The other authors have no conflicts of interest to declare.
Figures
References
LinkOut - more resources
Full Text Sources