

Human Herpes Virus 7-related encephalopathy in children
- PMID: 35441609
- PMCID: PMC9179060
- DOI: 10.23750/abm.v92iS4.12664
Human Herpes Virus 7-related encephalopathy in children
Abstract
Background: Primary HHV7 infection is almost ubiquitous, and it can present as exanthema subitem. Little is known on the clinical relevance of HHV7 neuroinvasion in immunocompetent children.
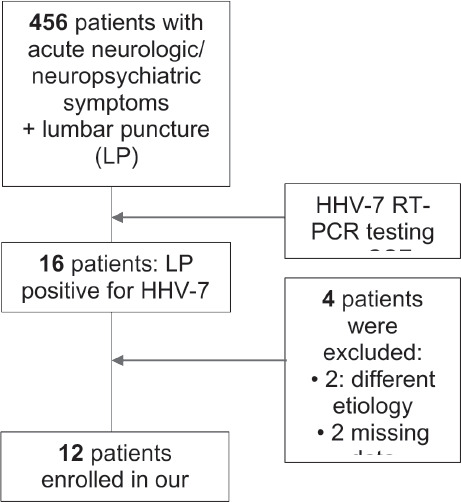
Methods: We describe 12 patients (median age 9.45 years, 50% males) with acute encephalopathy and active HHV7 infection. In all patients, HHV7-DNA was detected on cerebrospinal fluid (CSF) by RT-PCR.
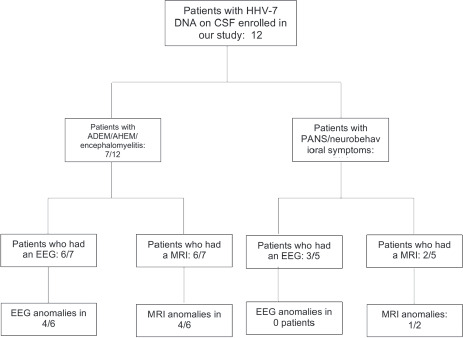
Results: 7/12 patients had meningoencephalitis (two with ADEM and one with MOG antibody-associated CIS); 5/12 showed acute neuropsychiatric symptoms. EEG showed anomalies exclusively in patients with meningoencephalitis. Six patients had RMN anomalies. CSF HHV7 copies ranged between 20 and 3,500 copies/mL (median 66 copies/mL) and mean HHV7 CSF/blood ratio was 0.75. Outcome was favorable in all children, although 3/12 had minor neurobehavioral sequelae. Mean follow-up period of 5.2 months.
Conclusions: HHV7 can determine neuroinvasion in immunocompetent children, leading to acute encephalopathy. Blood-brain barrier damage and high CSF/blood viral copies ratio correlated with a more severe presentation. We speculate on the importance of immune-mediated mechanisms in provoking clinical features.
Conflict of interest statement
Each author declares that he or she has no commercial associations (e.g. consultancies, stock ownership, equity interest, patent/licensing arrangement etc.) that might pose a conflict of interest in connection with the submitted article
Figures
References
-
- Kenneth J. Ryane. Sherris medical microbiology : an introduction to infectious diseases: Third edition. Norwalk, Conn. : Appleton & Lange. [1994] ©1994; 1994.
-
- Ward KN. The natural history and laboratory diagnosis of human herpesviruses-6 and -7 infections in the immunocompetent. J Clin Virol. 2005;32(3):183–193. - PubMed
-
- Huang LM, Lee CY, Liu MY, Lee PI. Primary infections of human herpesvirus-7 and herpesvirus-6: a comparative, longitudinal study up to 6 years of age. Acta Paediatr. 1997;86(6):604–608. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
