

Relationship between NAFLD and coronary artery disease: A Mendelian randomization study
- PMID: 35441719
- PMCID: PMC9970021
- DOI: 10.1002/hep.32534
Relationship between NAFLD and coronary artery disease: A Mendelian randomization study
Abstract
Background and aims: There is an ongoing debate on whether NAFLD is an active contributor or an innocent bystander in the pathogenesis of coronary artery disease (CAD). The aim of the present study was to assess the causal relationship between NAFLD and CAD.
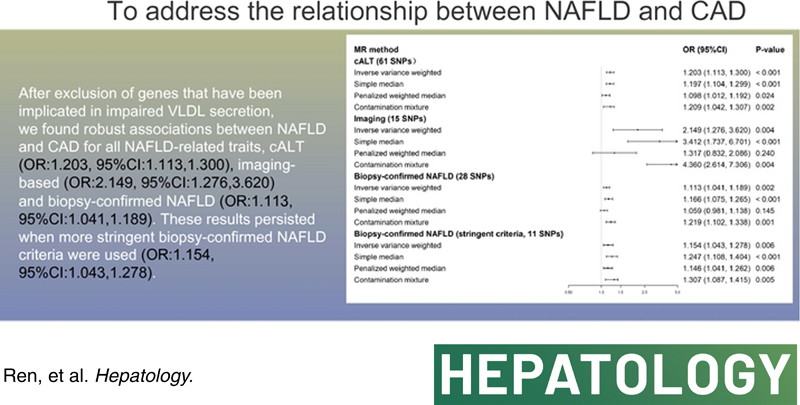
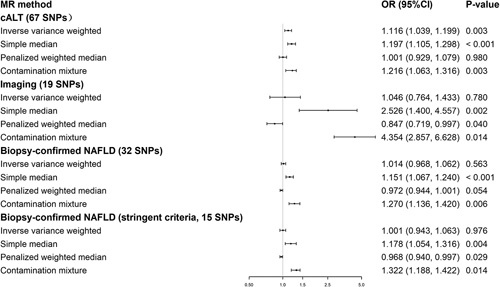
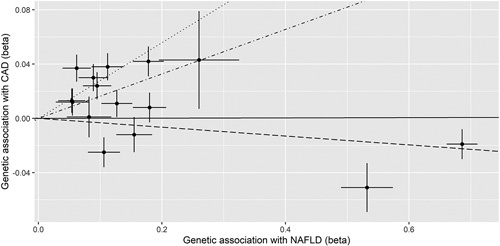
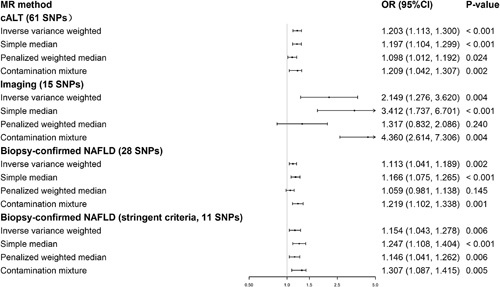
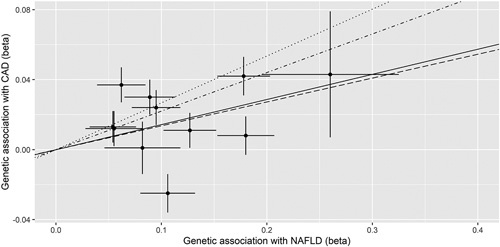
Approach and results: We performed two-sample Mendelian randomization (MR) analyses using summary-level data to assess the association between genetically predicted NAFLD (i.e., chronically elevated serum alanine aminotransferase levels [cALT], imaging-based and biopsy-confirmed NAFLD) and risk of CAD. Analyses were repeated after exclusion of NAFLD susceptibility genes that are associated with impaired VLDL secretion.Inverse-variance weighted MR analyses showed a statistically significant association between genetically predicted cALT and risk of CAD (OR: 1.116, 95% CI: 1.039, 1.199), but not for the other NAFLD-related traits (OR: 1.046, 95% CI: 0.764, 1.433 and OR: 1.014, 95% CI: 0.968, 1.062 for imaging-based and biopsy-confirmed NAFLD, respectively). MR-Egger regression revealed a statistically significant intercept, indicative of directional pleiotropy, for all traits. Repeat analyses after exclusion of genes associated with impaired VLDL secretion showed consistent associations between genetically predicted NAFLD and CAD for all traits (i.e., cALT [OR: 1.203, 95% CI: 1.113, 1.300]), imaging-based (OR: 2.149, 95% CI: 1.276, 3.620) and biopsy-confirmed NAFLD (OR: 1.113, 95% CI: 1.041, 1.189), which persisted when more stringent biopsy-confirmed NAFLD criteria were used (OR: 1.154, 95% CI: 1.043, 1.278) or when more stringent MR methods were applied. MR-Egger regression did not show a statistically significant intercept.
Conclusion: The two-sample MR analyses showed a robust association between genetically predicted NAFLD and CAD after exclusion of genetic variants that are implicated in impaired VLDL secretion.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors declare there are no conflicts of interest.
Figures
Comment in
-
Letter to the editor: Is NAFLD a bystander or contributor to coronary artery disease?Hepatology. 2022 Dec;76(6):E127-E128. doi: 10.1002/hep.32606. Epub 2022 Jul 21. Hepatology. 2022. PMID: 35689628 No abstract available.
References
-
- Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease—meta‐analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64:73–84. - PubMed
-
- European Association for the Study of the Liver (EASL). EASL‐EASD‐EASO Clinical Practice Guidelines for the management of non‐alcoholic fatty liver disease. J Hepatol. 2016;64:1388–402. - PubMed
-
- Younossi ZM, Stepanova M, Ong J, Trimble G, AlQahtani S, Younossi I, et al. . Nonalcoholic steatohepatitis is the most rapidly increasing indication for liver transplantation in the United States. Clin Gastroenterol Hepatol. 2021;19:580–89.e585. - PubMed
-
- Ong JP, Pitts A, Younossi ZM. Increased overall mortality and liver‐related mortality in non‐alcoholic fatty liver disease. J Hepatol. 2008;49:608–12. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
