

Effect of divergent continuous glucose monitoring technologies on glycaemic control in type 1 diabetes mellitus: A systematic review and meta-analysis of randomised controlled trials
- PMID: 35441743
- PMCID: PMC9542260
- DOI: 10.1111/dme.14854
Effect of divergent continuous glucose monitoring technologies on glycaemic control in type 1 diabetes mellitus: A systematic review and meta-analysis of randomised controlled trials
Abstract
Aims: We aimed to conduct a systematic review and meta-analysis of randomised controlled clinical trials (RCTs) assessing separately and together the effect of the three distinct categories of continuous glucose monitoring (CGM) systems (adjunctive, non-adjunctive and intermittently-scanned CGM [isCGM]), compared with traditional capillary glucose monitoring, on HbA1c and CGM metrics.
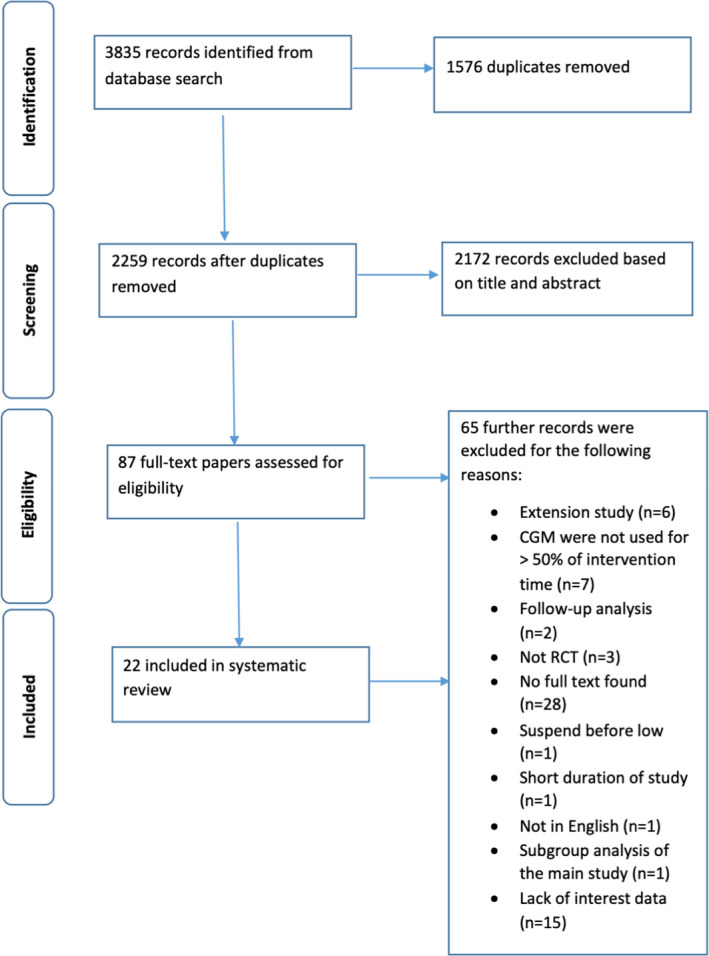
Methods: PubMed, Web of Science, Scopus and Cochrane Central register of clinical trials were searched. Inclusion criteria were as follows: randomised controlled trials; participants with type 1 diabetes of any age and insulin regimen; investigating CGM and isCGM compared with traditional capillary glucose monitoring; and reporting glycaemic outcomes of HbA1c and/or time-in-range (TIR). Glycaemic outcomes were extracted post-intervention and expressed as mean differences and 95%CIs between treatment and comparator groups. Results were pooled using a random-effects meta-analysis. Risk of bias was assessed using the Cochrane Rob2 tool.
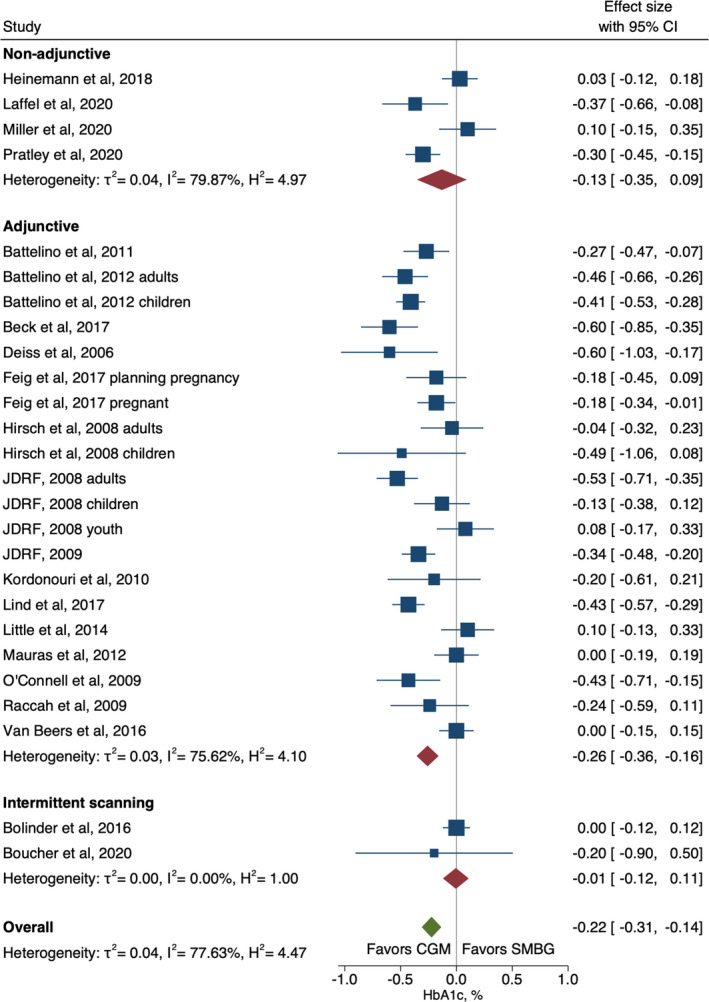
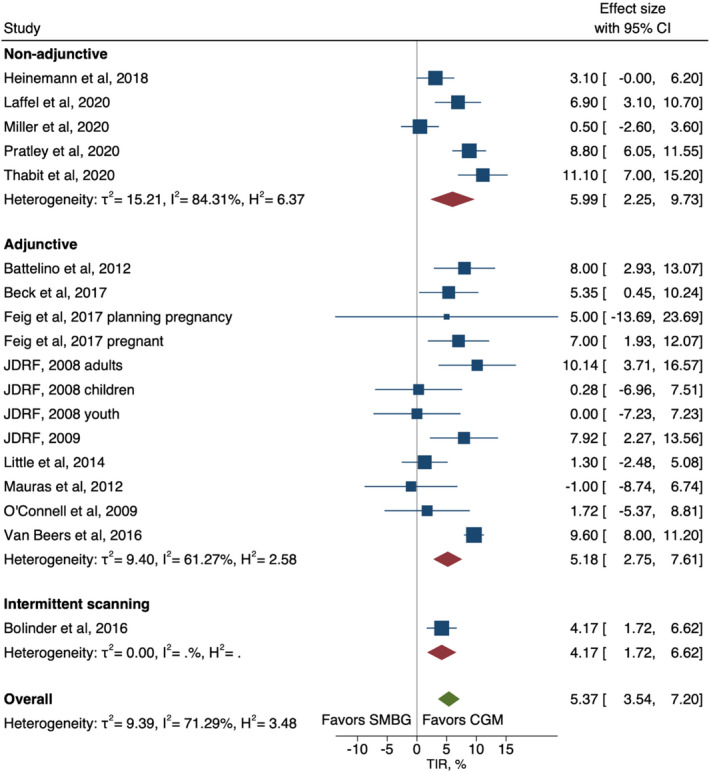
Results: This systematic review was conducted between January and April 2021; it included 22 RCTs (15 adjunctive, 5 non-adjunctive, and 2 isCGM)). The overall analysis of the pooled three categories showed a statistically significant absolute improvement in HbA1c percentage points (mean difference (95% CI): -0.22% [-0.31 to -0.14], I2 = 79%) for intervention compared with comparator and was strongest for adjunctive CGM (-0.26% [-0.36, -0.16]). Overall TIR (absolute change) increased by 5.4% (3.5 to 7.2), I2 = 71% for CGM intervention compared with comparator and was strongest with non-adjunctive CGM (6.0% [2.3, 9.7]).
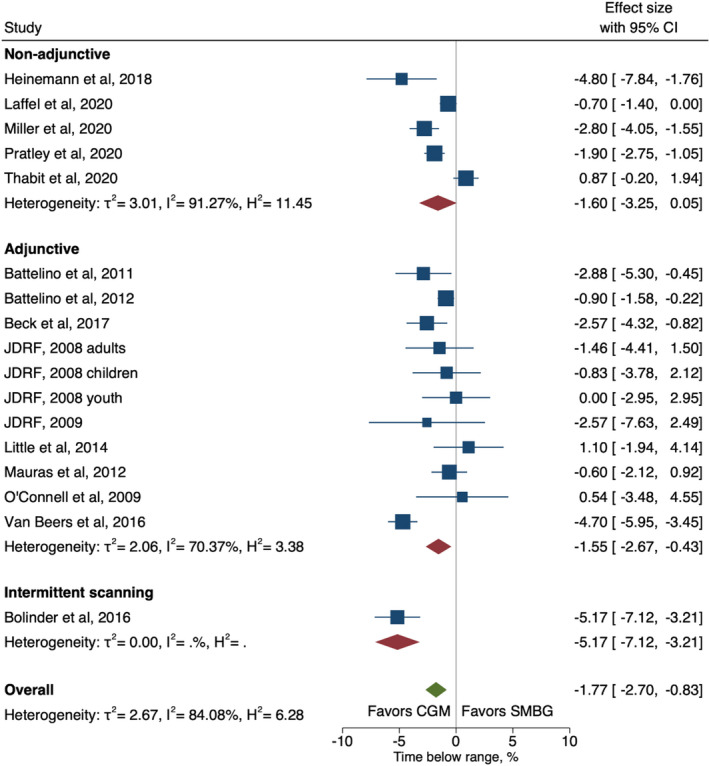
Conclusions: For individuals with T1D, use of CGM was beneficial for impacting glycaemic outcomes including HbA1c, TIR and time-below-range (TBR). Glycaemic improvement appeared greater for TIR for newer non-adjunctive CGM technology.
Keywords: CGM metrics; HbA1c; adjunctive CGM; continuous glucose monitoring; isCGM; non-adjunctive CGM; type 1 diabetes.
© 2022 The Authors. Diabetic Medicine published by John Wiley & Sons Ltd on behalf of Diabetes UK.
Conflict of interest statement
BJW has previously received research funding from Dexcom, Medtronic and iSENS. NO has received research funding from Dexcom, Roche Diabetes and Medtronic Diabetes and has participated in advisory boards for Dexcom, Roche Diabetes and Medtronic Diabetes. MIdB received Research funding from: Novo Nordisk, Medtronic, Dexcom, Pfizer and Research support from Medtronic, Dexcom, SOOIL, Honoraria from Medtronic. VNS reported receiving research supports through University of Colorado from Sanofi, Novo Nordisk, Eli‐Lilly, Insulet, Dexcom, Abbott, vTv Therapeutics, JDRF and NIH. VNS’ employer also received honoraria from Dexcom, insulet, Medscape and Sanofi for speaking, consulting or being on advisory board. ME, HS, JH, BG and SK declare no conflict of interest.
Figures
References
-
- Bloomgarden ZT. Type 1 diabetes and glucose monitoring. Diabet Care. 2007;30(11):2965‐2971. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
