

Systematic review of electrophysiology procedures in patients with obstruction of the inferior vena cava
- PMID: 35441755
- PMCID: PMC9323496
- DOI: 10.1111/jce.15505
Systematic review of electrophysiology procedures in patients with obstruction of the inferior vena cava
Abstract
Aims: The objective of the study was to conduct a systematic review to describe and compare the different approaches for performing cardiac electrophysiology (EP) procedures in patients with interrupted inferior vena cava (IVC) or equivalent entities causing IVC obstruction.
Methods: We conducted a structured search to identify manuscripts reporting EP procedures with interrupted IVC or IVC obstruction of any aetiology published up until August 2020. No restrictions were applied in the search strategy. We also included seven local cases that met inclusion criteria.
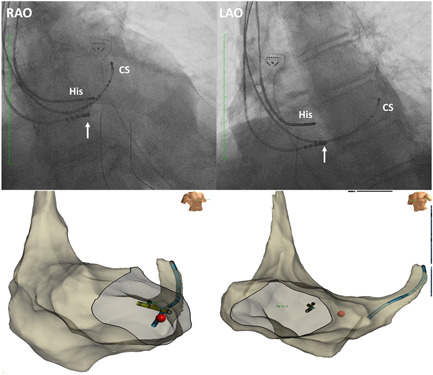
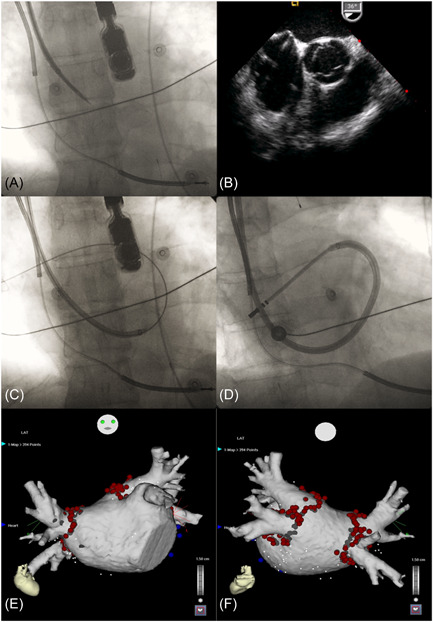
Results: The analysis included 142 patients (mean age 48.9 years; 48% female) undergoing 143 procedures. Obstruction of the IVC was not known before the index procedure in 54% of patients. Congenital interruption of IVC was the most frequent cause (80%); and, associated congenital heart disease (CHD) was observed in 43% of patients in this setting. The superior approach for ablation was the most frequently used strategy (52%), followed by inferior approach via the azygos or hemiazygos vein (24%), transhepatic approach (14%), and retroaortic approach (10%). Electroanatomical mapping (58%), use of long sheaths (41%), intracardiac echocardiography (19%), transesophageal echocardiography (15%) and remote controlled magnetic navigation (13%) were used as adjuncts to aid performance. Ablation was successful in 135 of 140 procedures in which outcomes were reported. Major complications were only reported in patients undergoing AF ablation, including two patients with pericardial effusion, one of whom required surgical repair, and another patient who died after inadvertent entry into an undiagnosed atrioesophageal fistula from a previous procedure.
Conclusion: The superior approach is most frequent approach for performing EP procedures in the setting of obstructed IVC. Transhepatic approach is a feasible alternative, and may provide a "familiar approach" for transseptal access when it is required. Adjunctive use of long sheaths, intravascular echocardiography, electro-anatomical mapping and remote magnetic navigation may be helpful, especially if there is associated complex CHD. With careful planning, EP procedures can usually be successfully performed with a low risk of complications.
Keywords: electrophysiology; inferior vena cava obstruction; interrupted inferior vena cava; superior approach; transhepatic approach.
© 2022 The Authors. Journal of Cardiovascular Electrophysiology published by Wiley Periodicals LLC.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures




Similar articles
-
Percutaneous transhepatic venous access for catheter ablation procedures in patients with interruption of the inferior vena cava.Circ Arrhythm Electrophysiol. 2011 Apr;4(2):235-41. doi: 10.1161/CIRCEP.110.960856. Epub 2011 Jan 26. Circ Arrhythm Electrophysiol. 2011. PMID: 21270102
-
Transseptal puncture and catheter ablation via the superior vena cava approach for persistent atrial fibrillation in a patient with polysplenia syndrome and interruption of the inferior vena cava: contact force-guided pulmonary vein isolation.Europace. 2017 Jul 1;19(7):1227-1232. doi: 10.1093/europace/euw095. Europace. 2017. PMID: 27174901
-
Double Inferior Vena Cava (IVC) With Intrahepatic Interruption, Hemiazygos Vein Continuation, and Intrahepatic Venous Shunt.Vasc Endovascular Surg. 2017 Jan;51(1):38-42. doi: 10.1177/1538574416687734. Vasc Endovascular Surg. 2017. PMID: 28100158
-
Congenital portosystemic venous connections and other abdominal venous abnormalities in patients with polysplenia and functionally univentricular heart disease: a case series and literature review.Congenit Heart Dis. 2011 Jan-Feb;6(1):28-40. doi: 10.1111/j.1747-0803.2010.00478.x. Congenit Heart Dis. 2011. PMID: 21269410 Review.
-
Successful blood sampling through azygos continuation with interrupted inferior vena cava. A case report and review of the literature.Int Heart J. 2011;52(5):327-30. doi: 10.1536/ihj.52.327. Int Heart J. 2011. PMID: 22008446 Review.
Cited by
-
Superior approach facilitated by atrial septoplasty in a case of persistent atrial fibrillation ablation with inferior vena caval obstruction.HeartRhythm Case Rep. 2024 May 28;10(8):564-567. doi: 10.1016/j.hrcr.2024.05.014. eCollection 2024 Aug. HeartRhythm Case Rep. 2024. PMID: 39155906 Free PMC article. No abstract available.
-
Atrial fibrillation ablation in a single atrium with inferior vena cava interruption.Ann Noninvasive Electrocardiol. 2023 Jul;28(4):e13057. doi: 10.1111/anec.13057. Epub 2023 Mar 31. Ann Noninvasive Electrocardiol. 2023. PMID: 37002650 Free PMC article.
-
Vascular Access and Closure Management for Electrophysiological Interventions: Small Interventions Big Impact.Curr Cardiol Rep. 2025 Jan 22;27(1):35. doi: 10.1007/s11886-024-02156-w. Curr Cardiol Rep. 2025. PMID: 39841329 Review.
-
Successful flutter catheter ablation through the azygos continuation due to an interrupted inferior vena cava.Radiol Case Rep. 2024 Aug 21;19(11):5094-5099. doi: 10.1016/j.radcr.2024.07.114. eCollection 2024 Nov. Radiol Case Rep. 2024. PMID: 39263502 Free PMC article.
-
Azygos vein approach for radiofrequency ablation of para-Hisian atrial tachycardia in a patient with inferior vena cava interruption.HeartRhythm Case Rep. 2025 Jan 24;11(4):343-346. doi: 10.1016/j.hrcr.2025.01.009. eCollection 2025 Apr. HeartRhythm Case Rep. 2025. PMID: 40486704 Free PMC article. No abstract available.
References
-
- Koc Z, Oguzkurt L. Interruption or congenital stenosis of the inferior vena cava: prevalence, imaging, and clinical findings. Eur J Radiol. 2007;62:257‐266. - PubMed
-
- Anderson RC, Adams P Jr., Burke B. Anomalous inferior vena cava with azygos continuation (infrahepatic interruption of the inferior vena cava). Report of 15 new cases. J Pediatr. 1961;59:370‐383. - PubMed
-
- Garg N, Agarwal BL, Modi N, Radhakrishnan S, Sinha N. Dextrocardia: an analysis of cardiac structures in 125 patients. Int J Cardiol. 2003;88:143‐155. - PubMed
-
- Arbelo E, Caballero E, Medina A. Successful slow pathway ablation for atrioventricular nodal re‐entrant tachycardia via a hypoplastic inferior vena cava in a patient with an azygos continuation. Europace. 2008;10:467‐468. - PubMed
-
- Metzner A, Chun KR, Kivelitz D, Kuck KH. Successful transseptal puncture and cryoballoon pulmonary vein isolation in adverse anatomy: interrupted inferior caval vein and azygos continuation. Circ Arrhythm Electrophysiol. 2009;2:e24‐e27. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
