

What Are the Benefits of Lateral Lumbar Interbody Fusion on the Treatment of Adult Spinal Deformity: A Systematic Review and Meta-Analysis Deformity
- PMID: 35442824
- PMCID: PMC9837508
- DOI: 10.1177/21925682221089876
What Are the Benefits of Lateral Lumbar Interbody Fusion on the Treatment of Adult Spinal Deformity: A Systematic Review and Meta-Analysis Deformity
Abstract
Study design: A systematic review and meta-analysis.
Objective: The purpose of this systematic review and meta-analysis was to compare the efficacy of lateral lumbar interbody fusion (LLIF) combined with posterior spinal fusion (PSF) with that of conventional PSF in the treatment of adult spinal deformity (ASD).
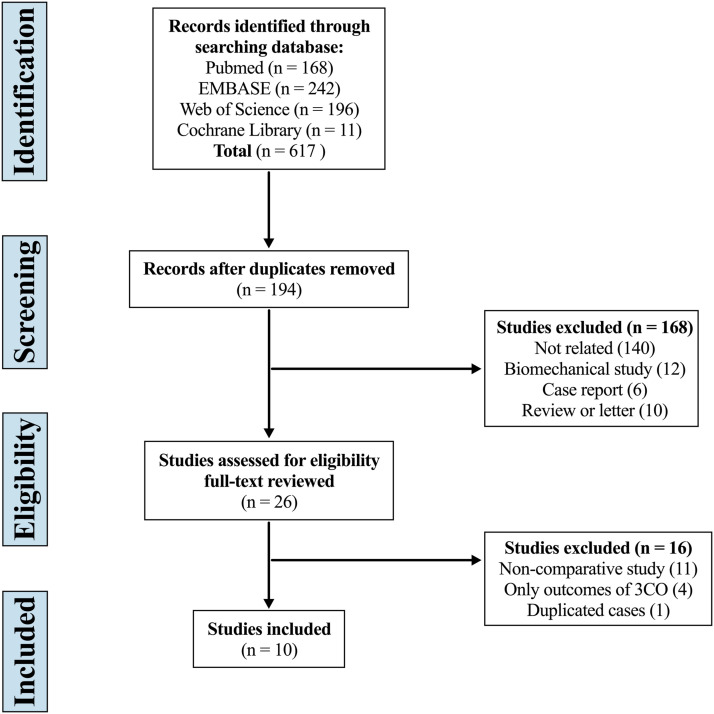
Methods: A comprehensive literature search was performed for relevant studies in PubMed, EMBASE, Web of Science, and the Cochrane Library. Spinopelvic parameters, surgical data, complications, and clinical outcomes at the last follow-up were compared between patients with ASD who underwent LLIF combined with PSF (LLIF+PSF group) and those who underwent conventional PSF (only-PSF group).
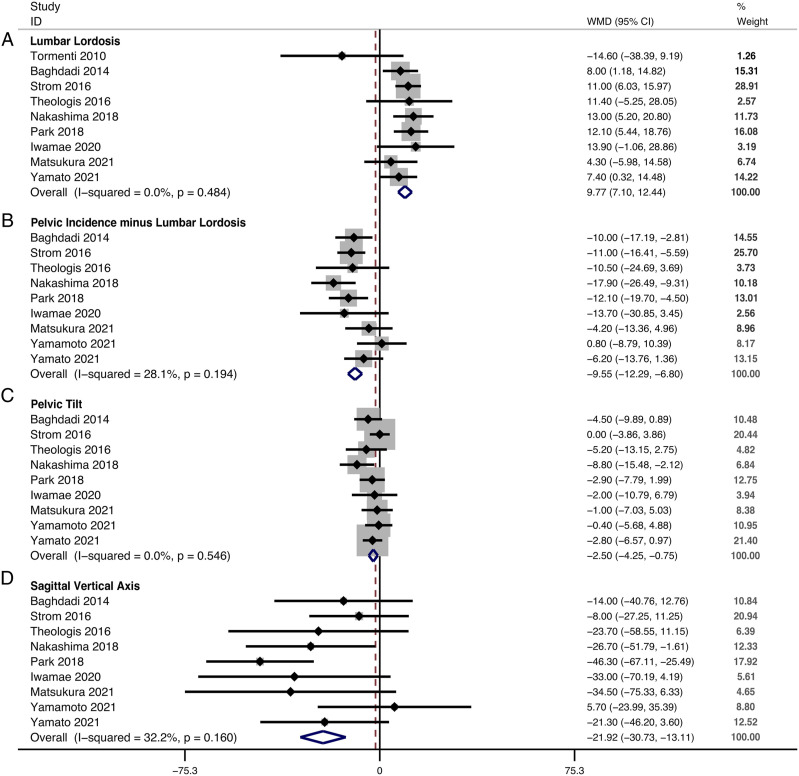
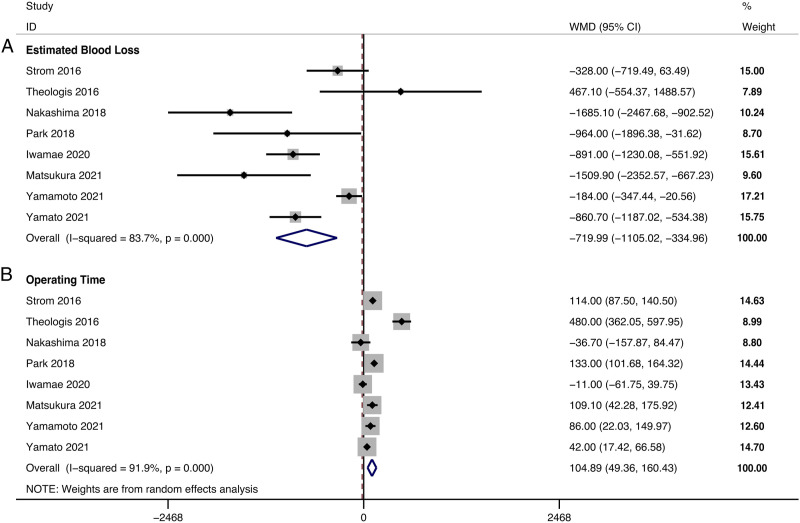
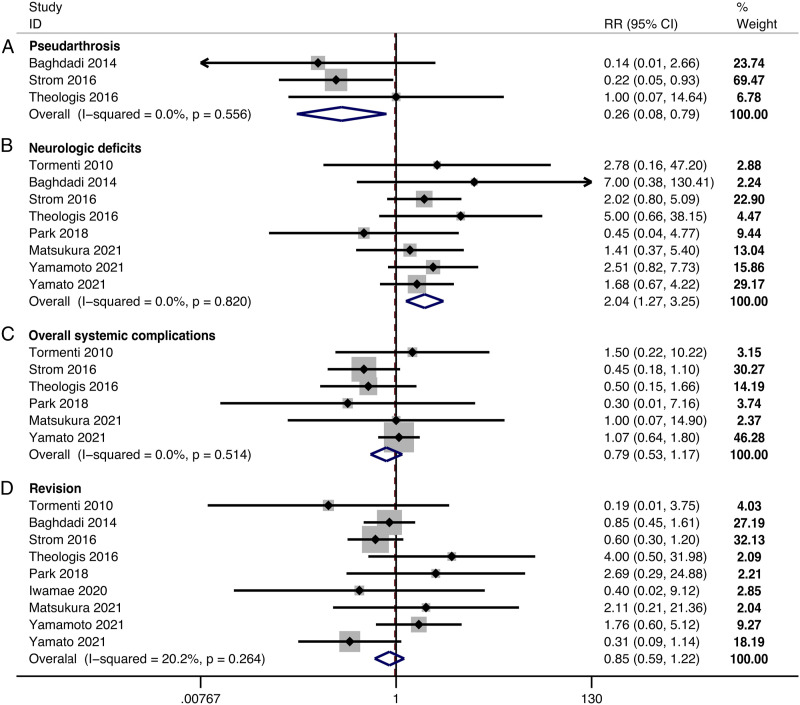
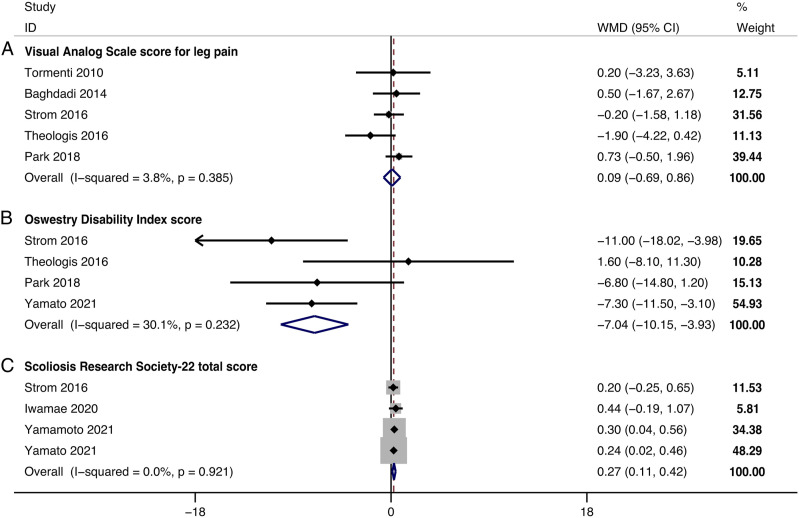
Results: Ten studies, comprising 621 patients with ASD (313 in the LLIF+PSF group and 308 in the only-PSF group), were included. The level of evidence was III for 7 studies and IV for 3 studies. There was no significant difference in the improvement in the visual analog scale score, systemic complication rate, and revision rate between groups. In the LLIF+PSF group, we noted a superior restoration of lumbar lordosis (weighted mean difference [WMD], 9.77; 95% confidence interval [CI] 7.10 to 12.44, P < .001), pelvic tilt (WMD, -2.50; 95% CI -4.25 to -.75, P = .005), sagittal vertical axis (WMD, -21.92; 95% CI -30.73 to -13.11, P < .001), and C7 plumb line-center sacral vertical line (WMD, -4.03; 95% CI -7.52 to -.54, P = .024); a lower estimated blood loss (WMD, -719.99; 95% CI -1105.02 to -334.96, P < .001) while a prolonged operating time (WMD, 104.89; 95% CI 49.36 to 160.43, P < .001); lower incidence of pseudarthrosis (risk ratio [RR], .26; 95% CI .08 to .79, P = .017) while higher incidence of neurologic deficits (RR, 2.04; 95% CI 1.27 to 3.25, P = .003); and a better improvement in Oswestry Disability Index score (WMD, -7.04; 95% CI -10.155 to -3.93, P < .001) and Scoliosis Research Society-22 total score (WMD, .27; 95% CI .11 to .42, P = .001). The level of evidence in this systematic review and meta-analysis was II.
Conclusion: Compared with conventional PSF, LLIF combined with PSF was associated with superior restoration of sagittal and coronal alignment, lower incidence of pseudarthrosis, better improvement in quality of life, and less surgical invasiveness in the treatment of ASD, albeit at the cost of prolonged surgical times and substantially high incidence of lower extremity symptoms. Surgeons should weigh the advantages and disadvantages of this procedure, and inform patients about its side effects.
Keywords: adult spinal deformity; lateral lumbar interbody fusion; posterior spinal fusion; spinopelvic parameters; surgical invasiveness.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Comparative analysis of 3 surgical strategies for adult spinal deformity with mild to moderate sagittal imbalance.J Neurosurg Spine. 2018 Jan;28(1):40-49. doi: 10.3171/2017.5.SPINE161370. Epub 2017 Nov 3. J Neurosurg Spine. 2018. PMID: 29087808
-
Utility of multilevel lateral interbody fusion of the thoracolumbar coronal curve apex in adult deformity surgery in combination with open posterior instrumentation and L5-S1 interbody fusion: a case-matched evaluation of 32 patients.J Neurosurg Spine. 2017 Feb;26(2):208-219. doi: 10.3171/2016.8.SPINE151543. Epub 2016 Oct 21. J Neurosurg Spine. 2017. PMID: 27767682
-
Efficacy of lateral lumbar interbody fusion combined with posterior spinal fusion compared with three-column osteotomy for adult spinal deformity with severe lumbar sagittal deformity.Eur J Orthop Surg Traumatol. 2022 Jul;32(5):973-979. doi: 10.1007/s00590-021-03068-z. Epub 2021 Jul 6. Eur J Orthop Surg Traumatol. 2022. PMID: 34228215
-
Is instrumented lateral lumbar interbody fusion superior to stand-alone lateral lumbar interbody fusion for the treatment of lumbar degenerative disease? A meta-analysis.J Clin Neurosci. 2021 Oct;92:136-146. doi: 10.1016/j.jocn.2021.08.002. Epub 2021 Aug 14. J Clin Neurosci. 2021. PMID: 34509241 Review.
-
Posterior minimally invasive scoliosis surgery versus the standard posterior approach for the management of adolescent idiopathic scoliosis: an updated meta-analysis.J Orthop Surg Res. 2022 Jan 29;17(1):58. doi: 10.1186/s13018-022-02954-4. J Orthop Surg Res. 2022. PMID: 35093152 Free PMC article. Review.
Cited by
-
Establishment of the prone transpsoas fusion surgery in Australia-a survey and analysis of major complications in early adopters.J Spine Surg. 2025 Mar 24;11(1):15-23. doi: 10.21037/jss-24-128. Epub 2025 Mar 11. J Spine Surg. 2025. PMID: 40242818 Free PMC article.
-
Comparative analysis of single-stage versus two-stage fusion surgeries for adult spinal deformity: radiographic outcomes, clinical improvements, and complication rates.Eur Spine J. 2025 Jul;34(7):2900-2907. doi: 10.1007/s00586-025-09036-z. Epub 2025 Jun 11. Eur Spine J. 2025. PMID: 40498330
-
Novel Combination of Lateral Interbody Fusion and Endoscopic Ipsi-Contra Decompression for Severe Stenosis From Lumbar Spondylolisthesis: A Case Report.Cureus. 2024 May 12;16(5):e60160. doi: 10.7759/cureus.60160. eCollection 2024 May. Cureus. 2024. PMID: 38868251 Free PMC article.
-
Factors and Experiences Associated With Unscheduled Hospital Readmission After Lateral Lumbar Interbody Fusion: A Case-Controlled Study.Orthop Surg. 2025 May;17(5):1389-1396. doi: 10.1111/os.70022. Epub 2025 Mar 16. Orthop Surg. 2025. PMID: 40091307 Free PMC article.
-
Expandable cages that expand both height and lordosis provide improved immediate effect on sagittal alignment and short-term clinical outcomes following minimally invasive transforaminal lumbar interbody fusion (MIS TLIF).J Spine Surg. 2024 Mar 20;10(1):55-67. doi: 10.21037/jss-23-106. Epub 2024 Mar 15. J Spine Surg. 2024. PMID: 38567017 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
