

Gastrointestinal Kohlmeier-Degos disease: a narrative review
- PMID: 35443671
- PMCID: PMC9022239
- DOI: 10.1186/s13023-022-02322-9
Gastrointestinal Kohlmeier-Degos disease: a narrative review
Abstract
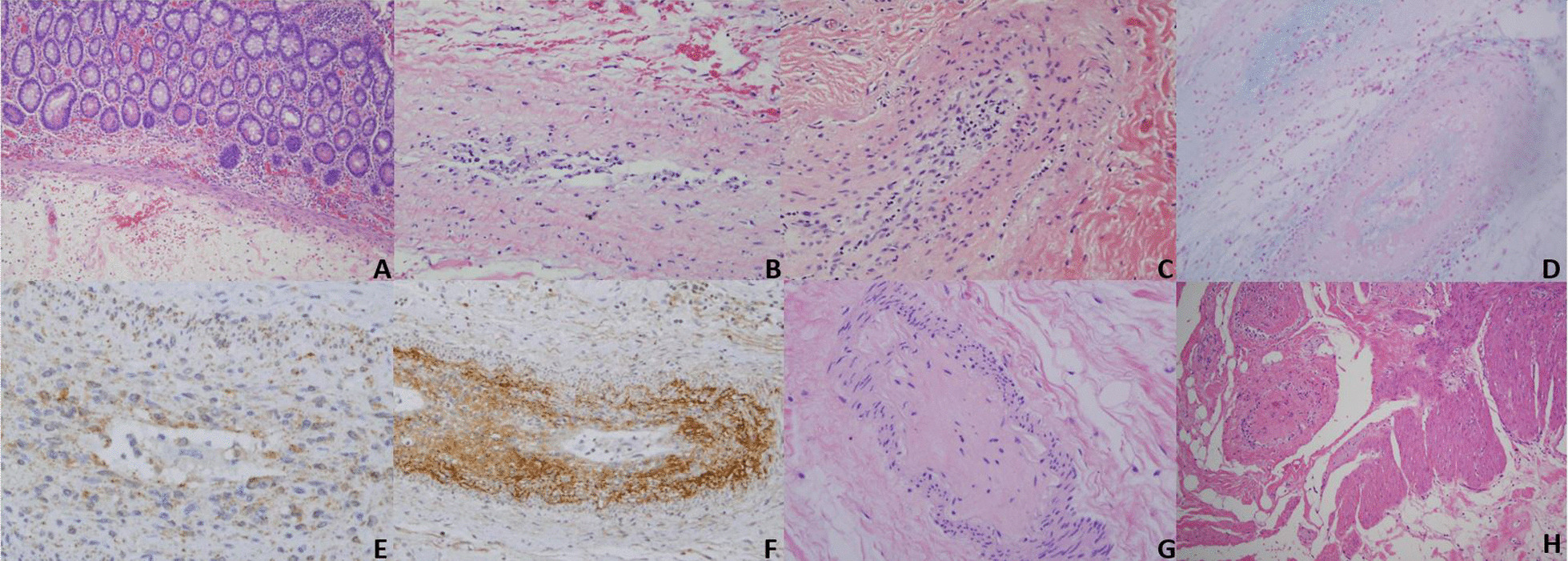
Introduction: Kohlmeier-Degos (K-D) disease is a rare obliterative vasculopathy that can present as a benign cutaneous form or with potentially malignant systemic involvement. The gastrointestinal tract is most frequently involved in systemic disease and mortality is often related to bowel perforations. Herein, we provide information to providers and patients regarding gastrointestinal K-D symptomology, pathology, treatment, and diagnosis, with a focus on the importance of timely diagnostic laparoscopy. We present three new cases of gastrointestinal K-D to highlight varying disease presentations and outcomes. BODY: Based on reviewed reports, perforation is preceded by at least one gastrointestinal symptom: abdominal pain/cramping, anorexia/weight loss, vomiting, diarrhea, nausea, gastrointestinal bleeding, obstipation, constipation, and abdominal fullness. Perforation most commonly occurs in the small intestine and often results in sepsis and death. Although underutilized, laparoscopy is the most sensitive and specific diagnostic technique, demonstrating serosal porcelain plaques similar to those on the skin and characteristic for K-D. The combination of eculizumab and treprostinil is presently the most effective treatment option for gastrointestinal K-D. The pathology of gastrointestinal K-D is characterized by an obliterative intimal arteriopathy eventuating in occlusive acellular deposits of mucin and collagen along with an extravascular pauci-cellular sclerosing process resembling scleroderma confined to the subserosal fat. C5b-9 and interferon-alpha are both expressed in all caliber of vessels in the affected intestine. While C5b-9 blockade does not prevent the intimal expansion, enhanced type I interferon signaling is likely a key determinant to intimal expansion by, causing an influx of monocytes which transdifferentiate into procollagen-producing myofibroblast-like cells.
Conclusion: Prompt laparoscopic evaluation is necessary in any K-D patient with an abdominal symptom to facilitate diagnosis and treatment initiation, as well as to hopefully decrease mortality. Those with gastrointestinal K-D should start on eculizumab as soon as possible, as onset of action is immediate.
Keywords: C5b-9; Degos disease; Eculizumab; Gastrointestinal; Interferon; Kohlmeier–Degos disease; Laparoscopy; Perforation; Treprostinil.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Toledo AE, Shapiro LS, Farrell JF, Magro CM, Polito J. Laparoscopy shows superiority over endoscopy for early detection of malignant atrophic papulosis gastrointestinal complications: a case report and review of literature. BMC Gastroenterol. 2015;15:156. doi: 10.1186/s12876-015-0387-y. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
