

China Stroke Statistics: an update on the 2019 report from the National Center for Healthcare Quality Management in Neurological Diseases, China National Clinical Research Center for Neurological Diseases, the Chinese Stroke Association, National Center for Chronic and Non-communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention and Institute for Global Neuroscience and Stroke Collaborations
- PMID: 35443985
- PMCID: PMC9614174
- DOI: 10.1136/svn-2021-001374
China Stroke Statistics: an update on the 2019 report from the National Center for Healthcare Quality Management in Neurological Diseases, China National Clinical Research Center for Neurological Diseases, the Chinese Stroke Association, National Center for Chronic and Non-communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention and Institute for Global Neuroscience and Stroke Collaborations
Abstract
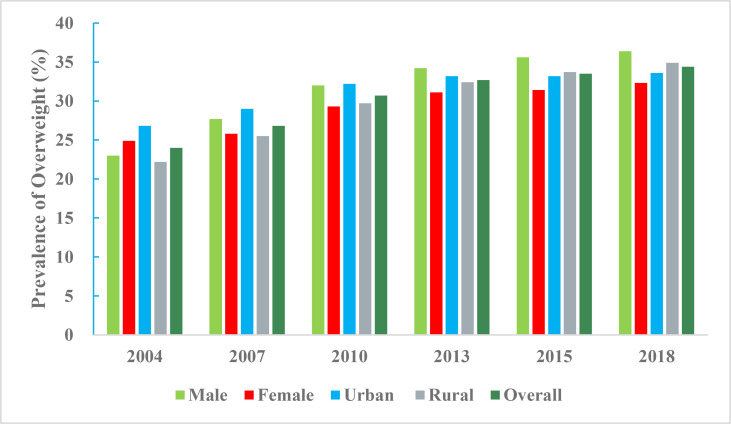
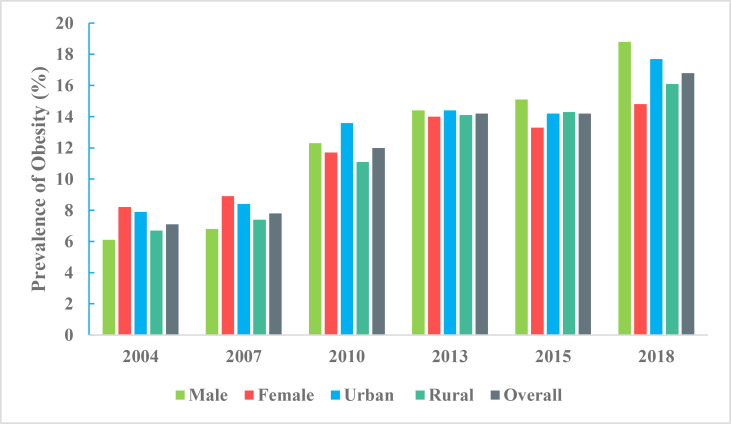
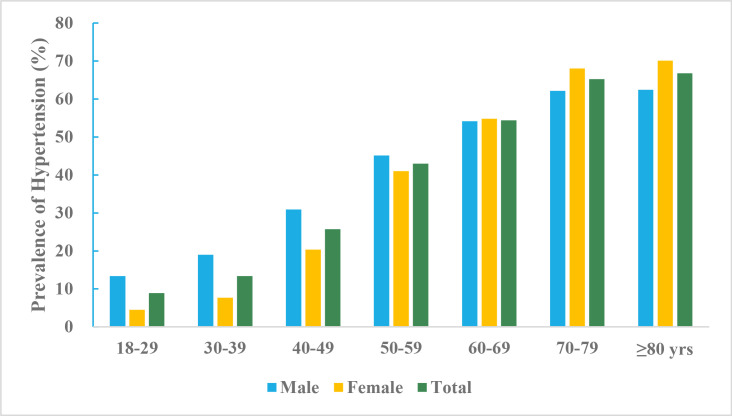
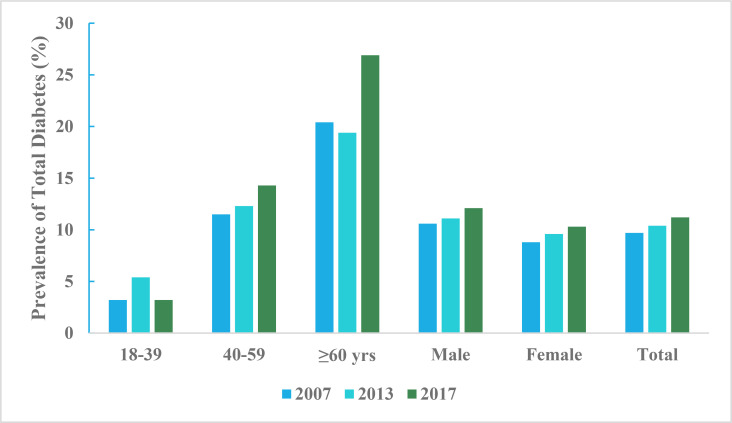
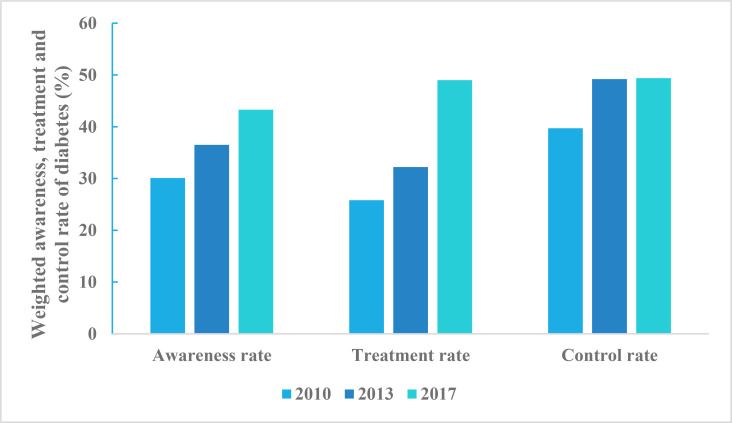
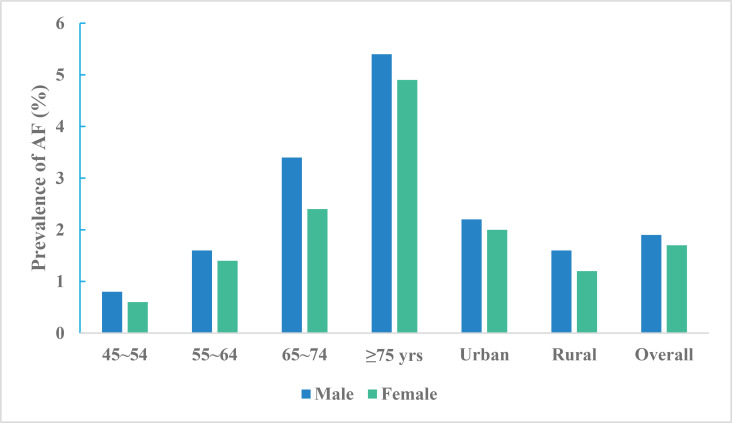
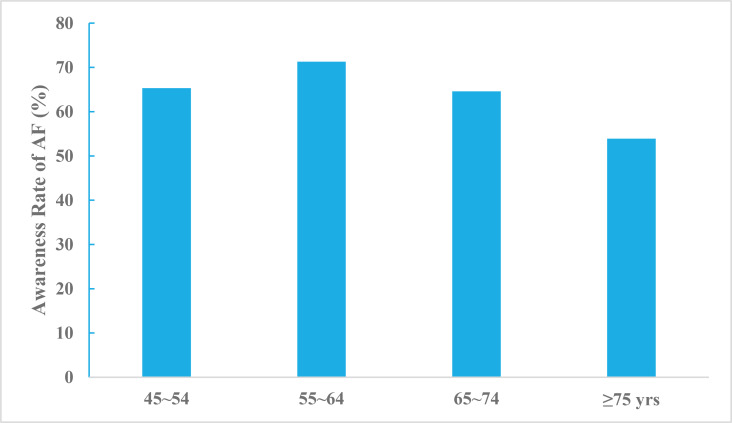
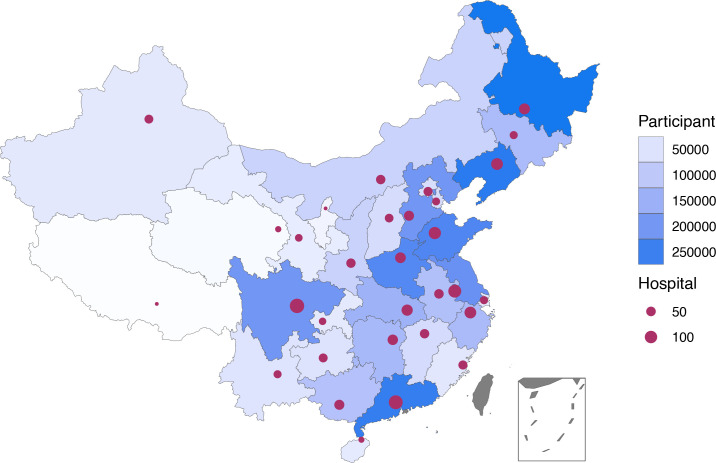
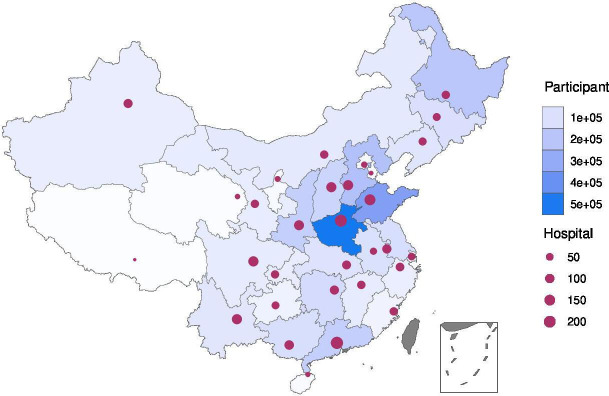
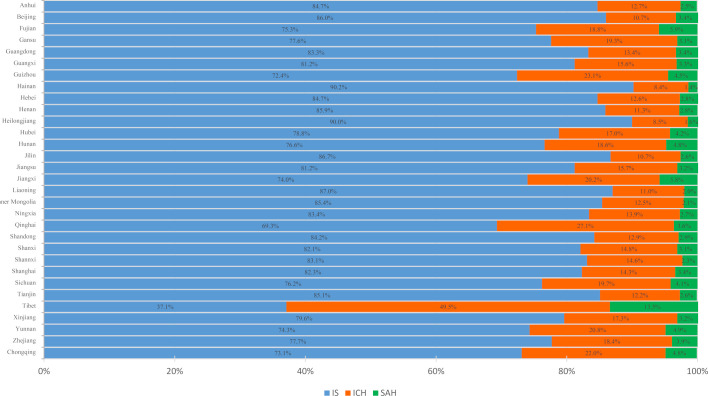
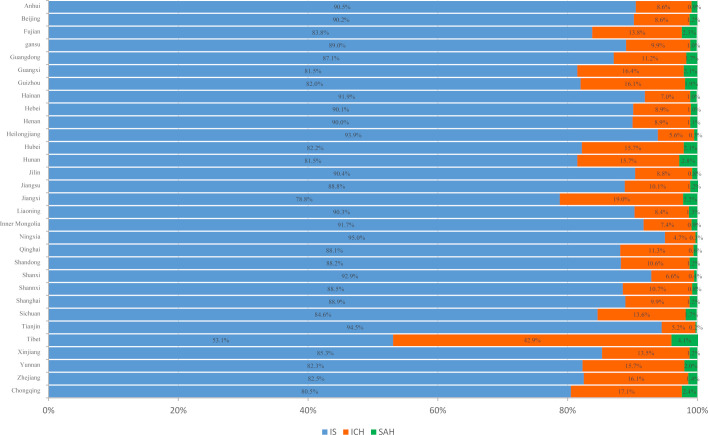
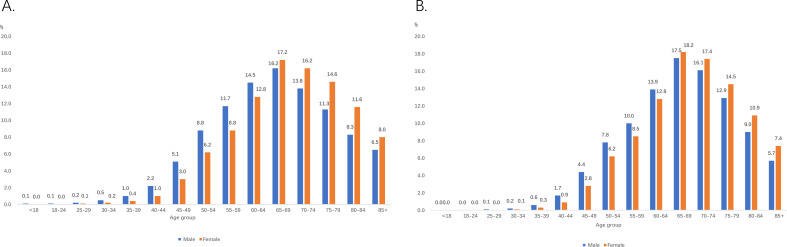
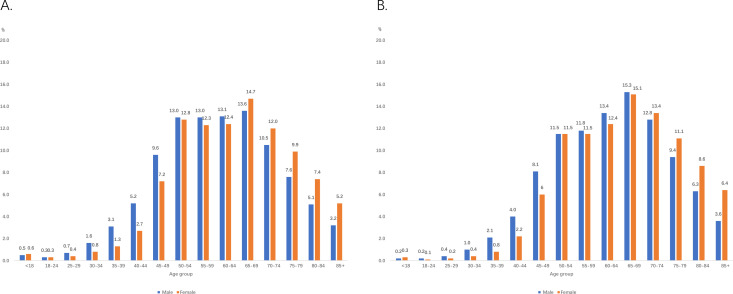
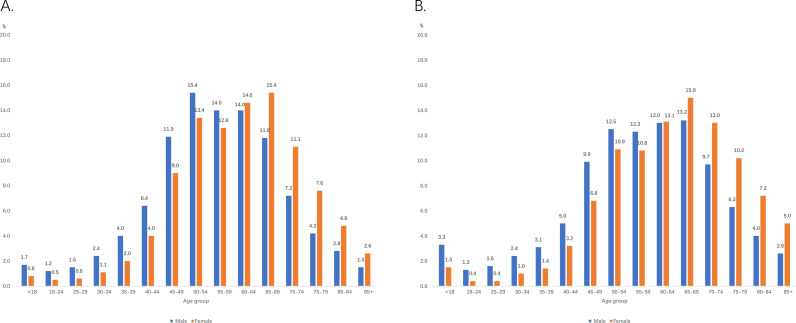
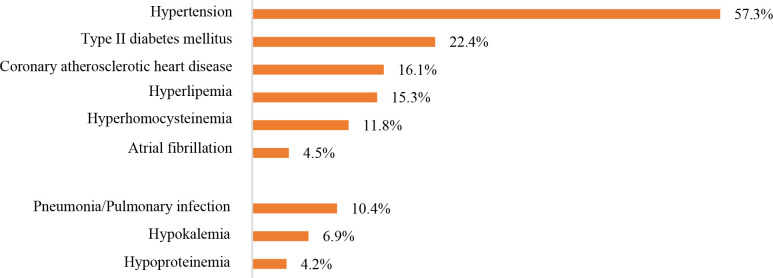
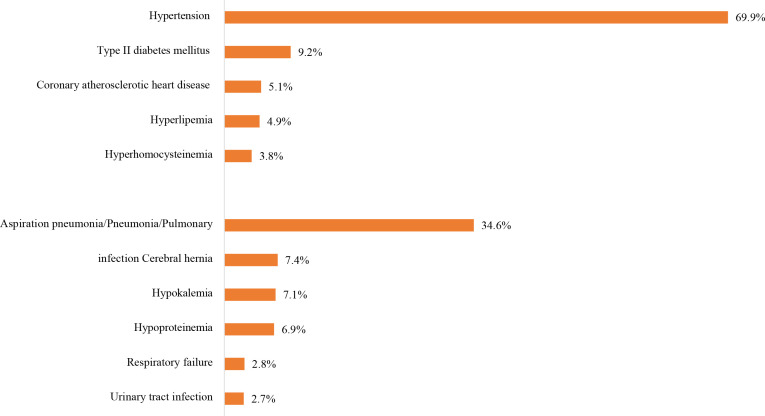
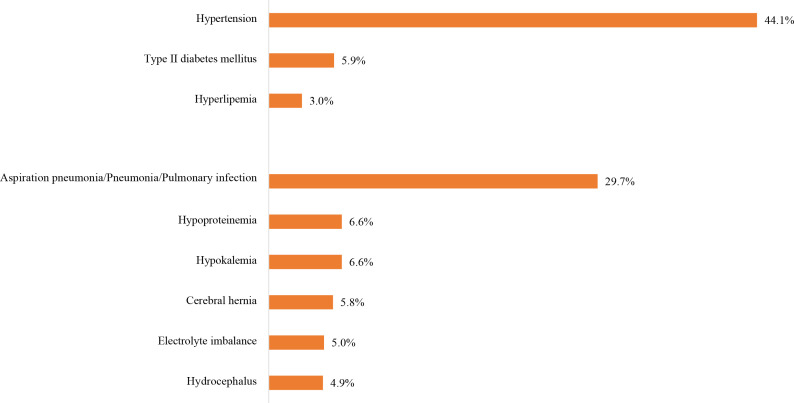
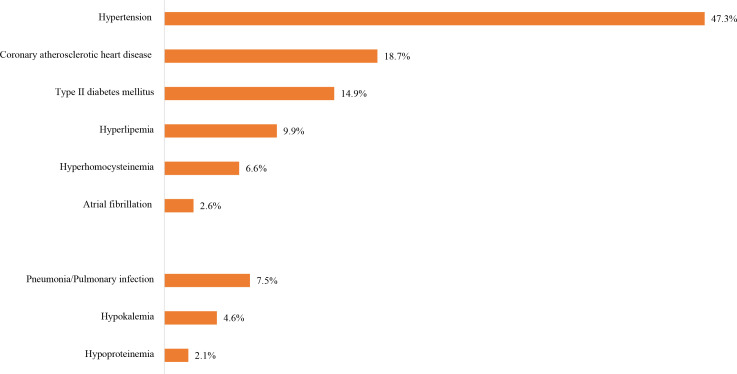
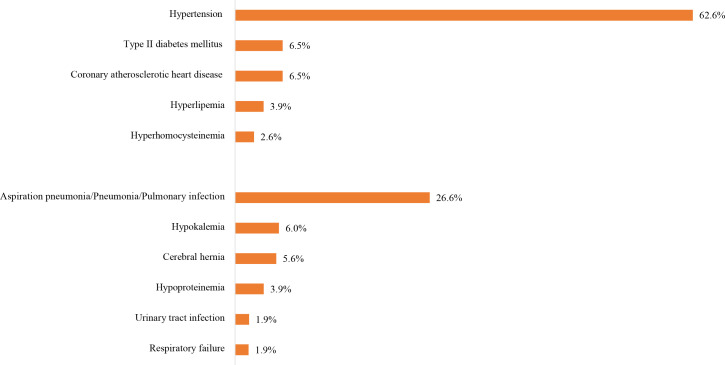
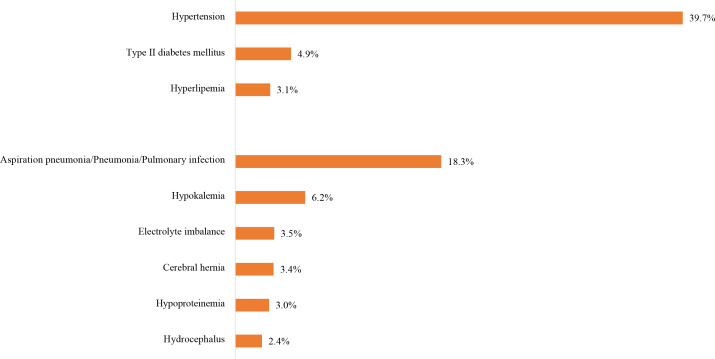
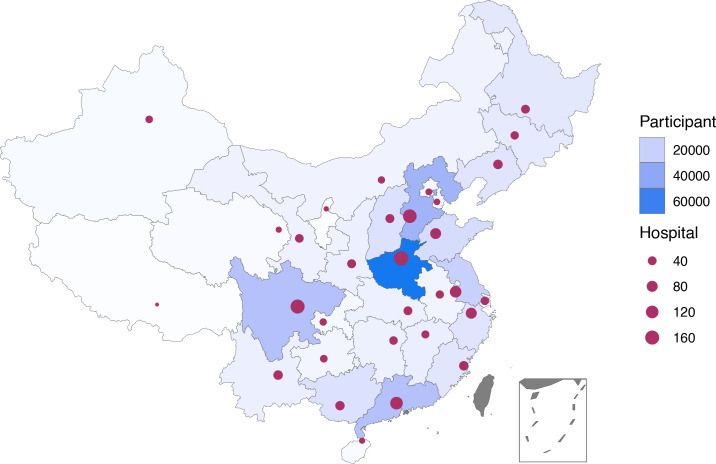
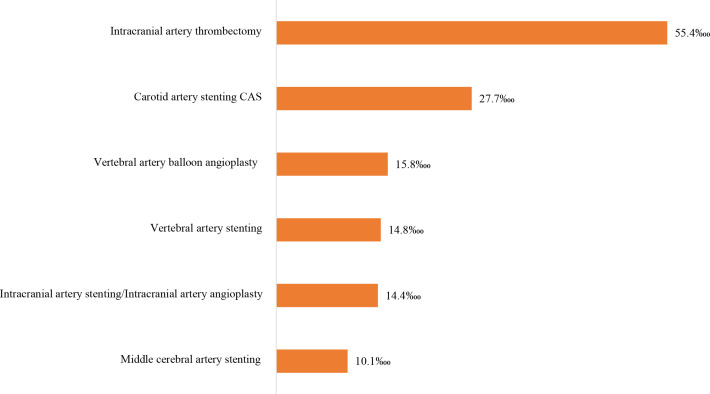
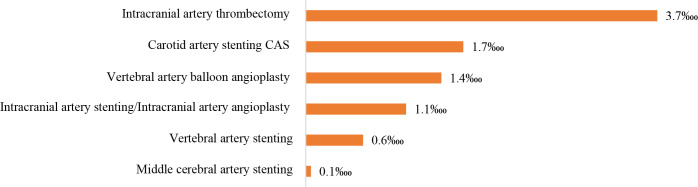
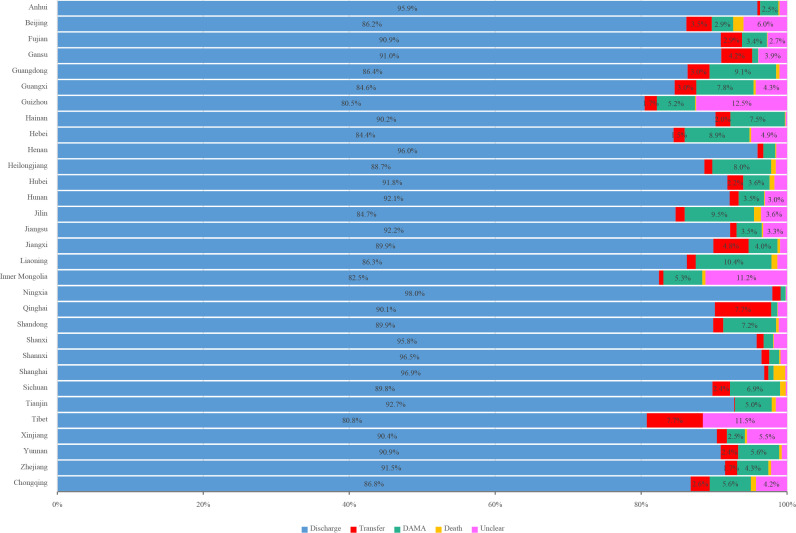
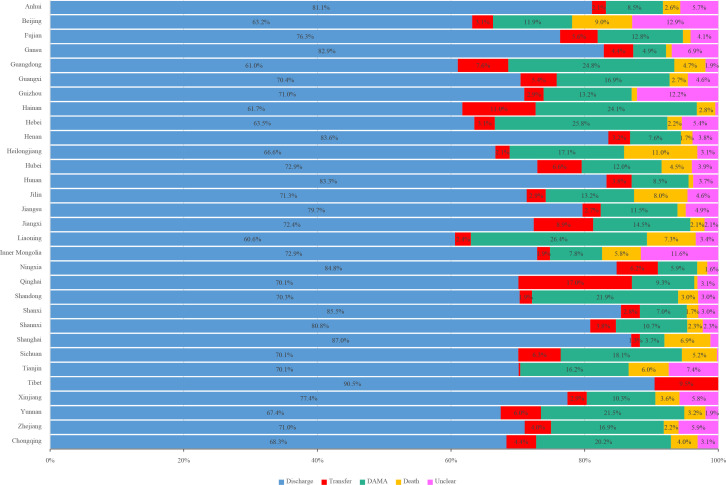
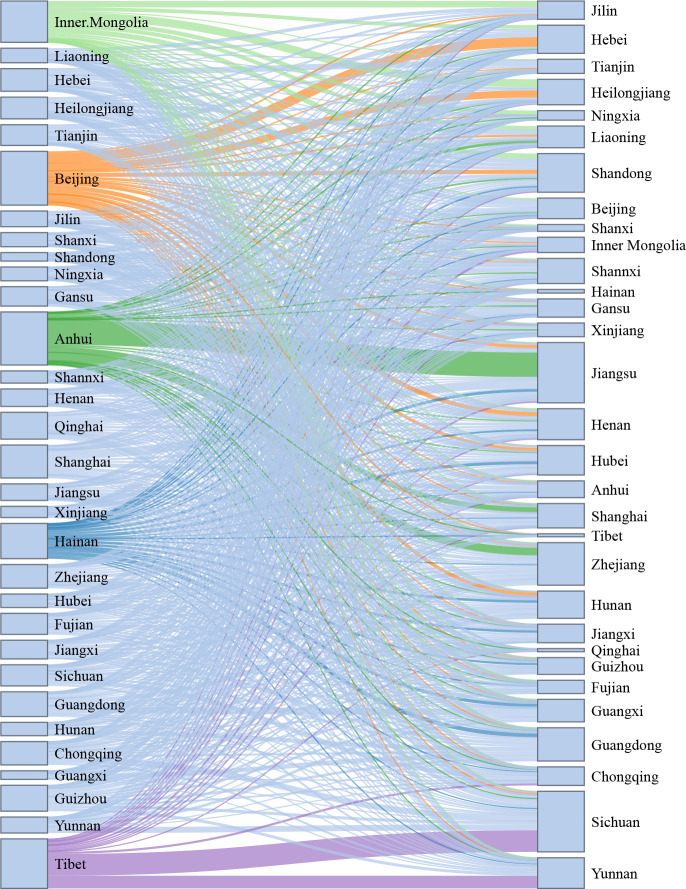
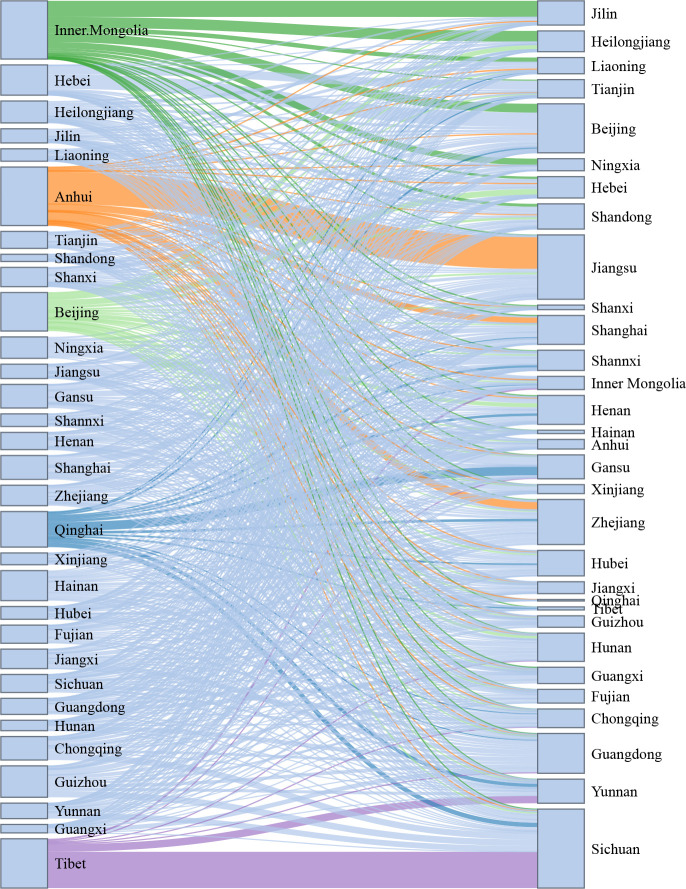
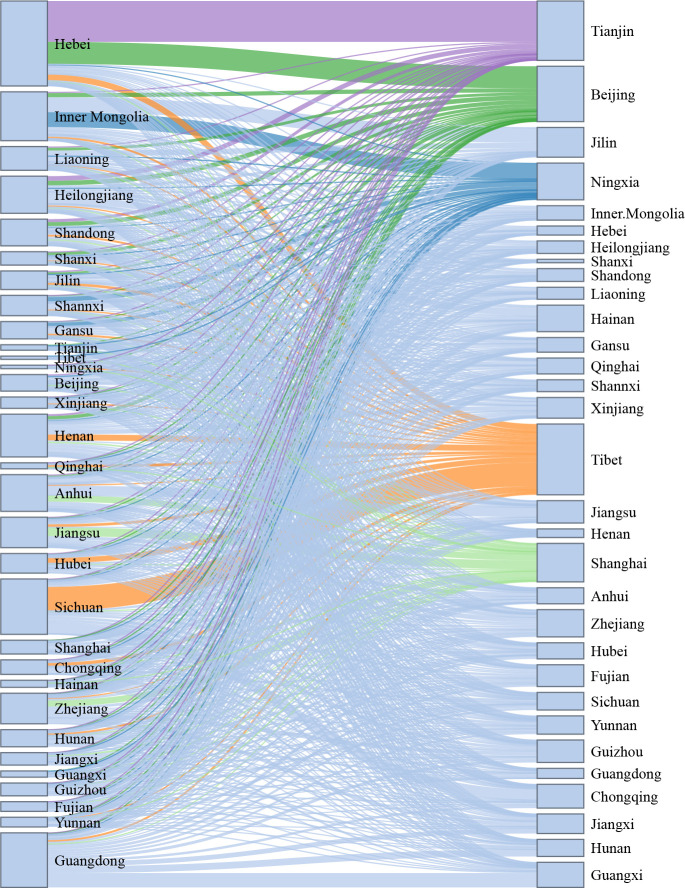
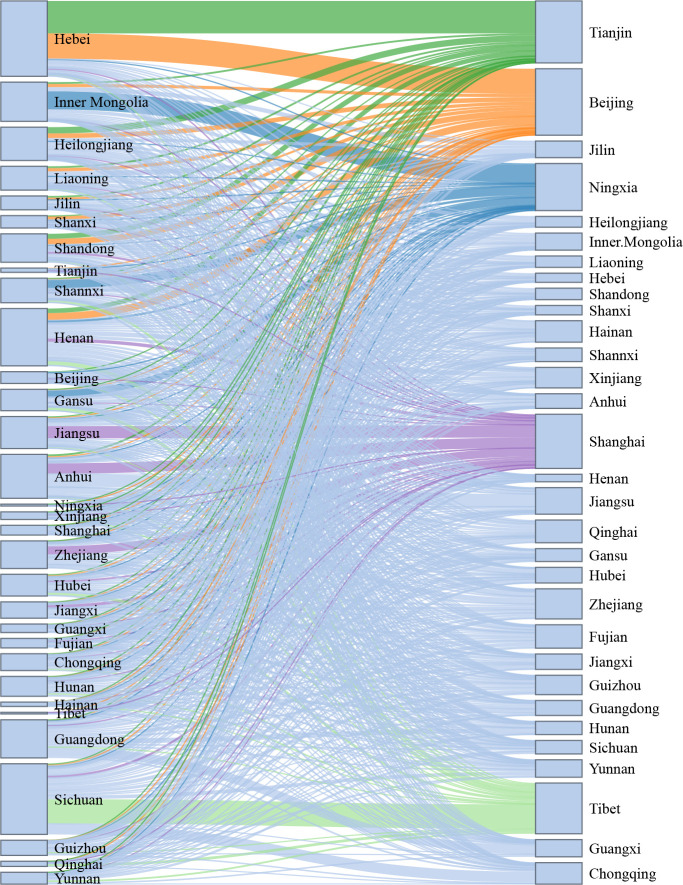
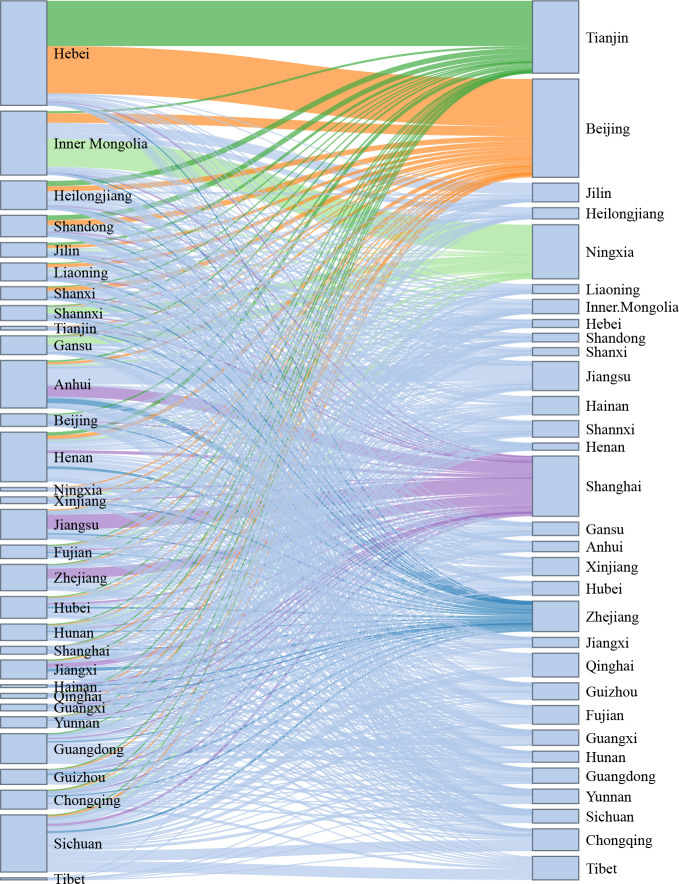
China faces the greatest challenge from stroke in the world. According to results from the Global Burden of Disease Study 2019, there were 3.94 million new stroke cases, 28.76 million prevalent cases and 2.19 million deaths due to stroke in China in 2019. Furthermore, stroke is also the leading cause of disability-adjusted life-year (DALY) in China, the number of DALYs reached 45.9 million in 2019. Several recent large-scale epidemiological surveys have updated the data on pre-existing conditions contributed to stroke. The age-adjusted prevalence of overweight among Chinese adults aged 18-69 years was 34.4%, and the prevalence of obesity was 16.8% in 2018. 50.9% of Chinese adults ≥18 years of age without history of hypertension had prehypertension in 2018. The weighted prevalence of hypertension in adults was 27.5% in 2018. The weighted prevalence of total diabetes and pre-diabetes diagnosed by the American Diabetes Association criteria were 12.8% and 35.2%, respectively, among Chinese adults ≥18 years of age in 2017. The weighted atrial fibrillation prevalence was 1.8% among Chinese adults ≥45 years of age and equates to being present in an estimated 7.9 million people in China. Data from 1672 tertiary public hospitals in the Hospital Quality Monitoring System (HQMS) showed that 3 411 168 stroke cases were admitted during 2019. Of those, 2 818 875 (82.6%) were ischaemic strokes (ISs), 485 474 (14.2%) were intracerebral haemorrhages (ICHs), 106 819 (3.1%) were subarachnoid haemorrhages (SAHs). The average age was 66 years old, and 59.6% were male. A total of 1379 (<0.1%), 2604 (0.5%), 1250 (1.2%) paediatric strokes (age <18 years) were identified among IS, ICH and SAH, respectively. Over one-third (1 231 519 (36.1%)) of the stroke cases were covered by urban resident basic medical insurance, followed by urban employee basic medical insurance (891 103 (26.1%)) and new rural cooperative medical schema (543 108 (15.9%)). The leading risk factor was hypertension (57.3% for IS, 69.9% for ICH and 44.1% for SAH), and the leading comorbidity was pneumonia or pulmonary infection (10.4% for IS, 34.6% for ICH and 29.7% for SAH). In-hospital death/discharge against medical advice rate was 8.5%, ranging from 6.0% for IS to 20.6% for SAH. The median and IQR of length of stay was 9.0 (6.0-13.0) days, ranging from 10.0 (7.0-13.0) in IS to 14.0 (8.0-22.0) in ICH. Similar data from 2847 secondary public hospitals or private hospitals in the HQMS were also reported. Data from HQMS showed that higher proportions of interprovincial admission to other provinces were seen in Inner Mongolia, Anhui, Tibet and Beijing. Higher proportions of interprovincial admission from other provinces were seen in Beijng, Tianjin, Shanghai and Ningxia. Data from 323 601 strokes from 1337 hospitals in the Chinese Stroke Center Alliance during 2019 demonstrated that the composite scores of guideline-recommended key performance indicators for patients with IS, ICH and SAH were 0.78±0.20, 0.69±0.27 and 0.60±0.31, respectively.
Keywords: stroke.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures



References
-
- Zhou M, Xue M. Annual data set on national mortality surveillance 2019. Beijing: China Science and Technology Press, 2020.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical