

Predictors and predictive effects of acute pain trajectories after gastrointestinal surgery
- PMID: 35444171
- PMCID: PMC9021210
- DOI: 10.1038/s41598-022-10504-5
Predictors and predictive effects of acute pain trajectories after gastrointestinal surgery
Abstract
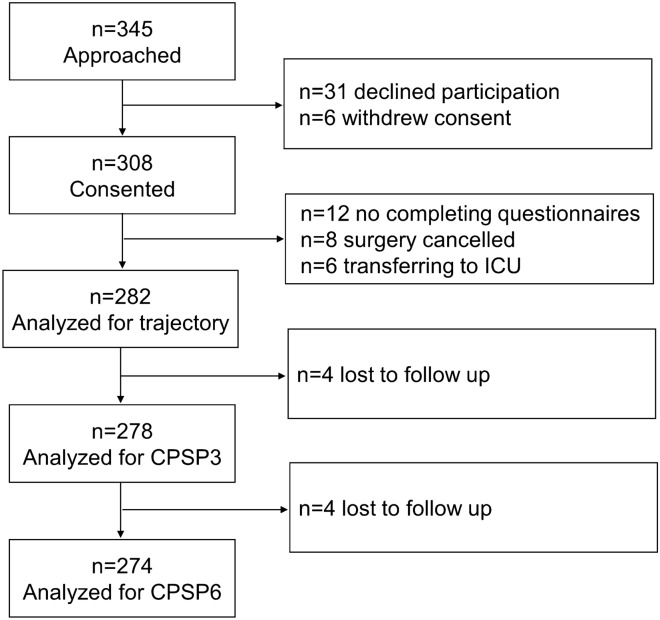
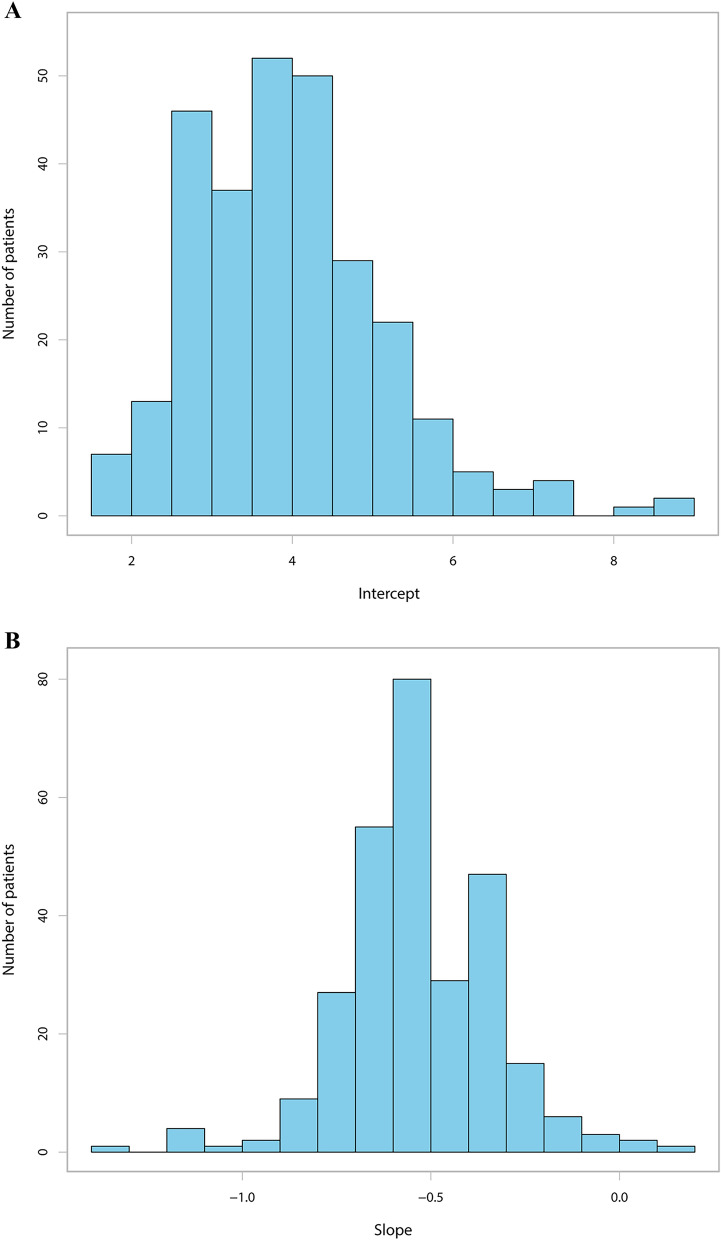
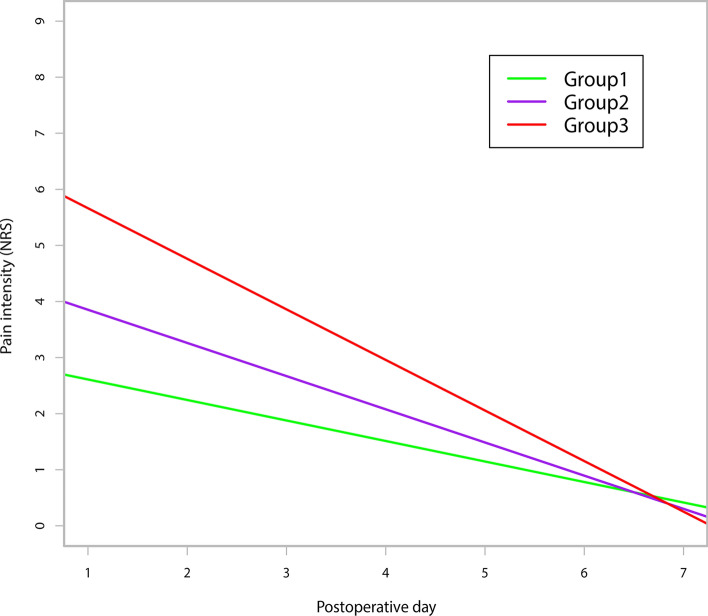
Few studies have investigated factors associated with acute postsurgical pain (APSP) trajectories, and whether the APSP trajectory can predict chronic postsurgical pain (CPSP) remains unclear. We aimed to identify the predictors of APSP trajectories in patients undergoing gastrointestinal surgery. Moreover, we hypothesised that APSP trajectories were independently associated with CPSP. We conducted a prospective cohort study of 282 patients undergoing gastrointestinal surgery to describe APSP trajectories. Psychological questionnaires were administered 1 day before surgery. Meanwhile, demographic characteristics and perioperative data were collected. Average pain intensity during the first 7 days after surgery was assessed by a numeric rating scale (NRS). Persistent pain intensity was evaluated at 3 and 6 months postoperatively by phone call interview. CPSP was defined as pain at the incision site or surrounding areas of surgery with a pain NRS score ≥ 1 at rest. The intercept and slope were calculated by linear regression using the least squares method. The predictors for the APSP trajectory and CPSP were determined using multiple linear regression and multivariate logistic regression, respectively. Body mass index, morphine milligram equivalent (MME) consumption, preoperative chronic pain and anxiety were predictors of the APSP trajectory intercept. Moreover, MME consumption and preoperative anxiety could independently predict the APSP trajectory slope. The incidence of CPSP at 3 and 6 months was 30.58% and 16.42% respectively. APSP trajectory and age were predictors of CPSP 3 months postoperatively, while female sex and preoperative anxiety were predictive factors of CPSP 6 months postoperatively. Preoperative anxiety and postoperative analgesic consumption can predict APSP trajectory. In addition, pain trajectory was associated with CPSP. Clinicians need to stay alert for these predictors and pay close attention to pain resolution.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Vaurio LE, Sands LP, Wang Y, Mullen EA, Leung JM. Postoperative delirium: The importance of pain and pain management. Anesth. Analg. 2006;102:1267–1273. doi: 10.1213/01.ane.0000199156.59226.af. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
