

Causal mapping of human brain function
- PMID: 35444305
- PMCID: PMC9387758
- DOI: 10.1038/s41583-022-00583-8
Causal mapping of human brain function
Abstract
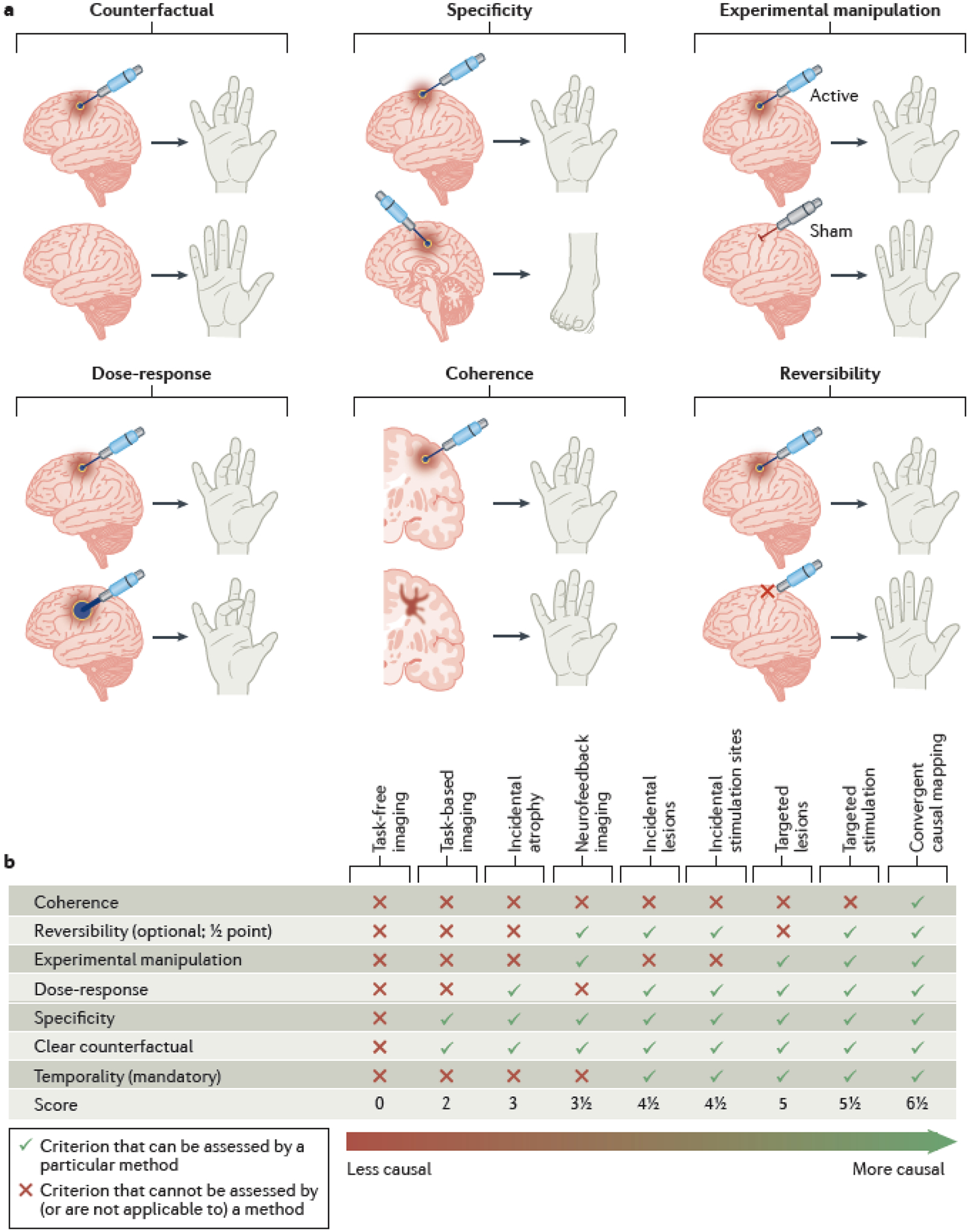
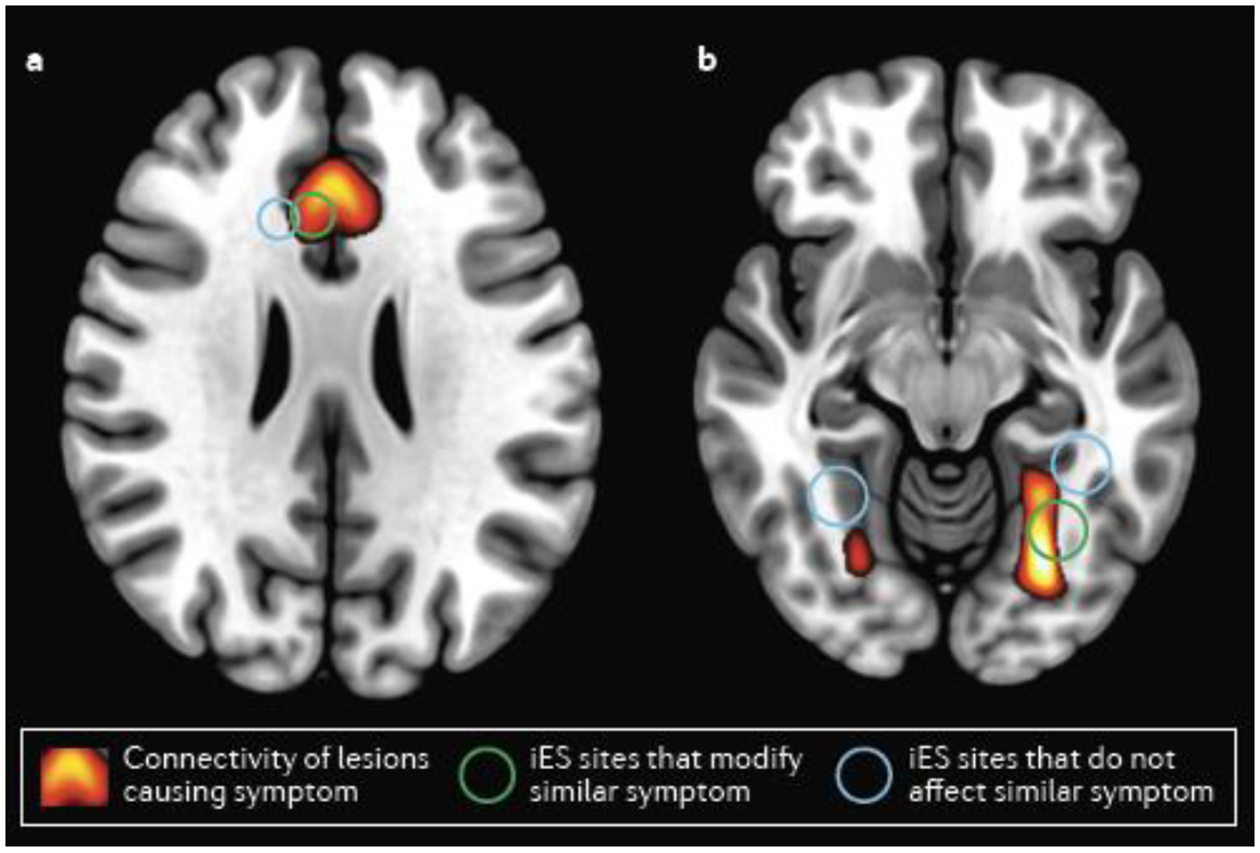
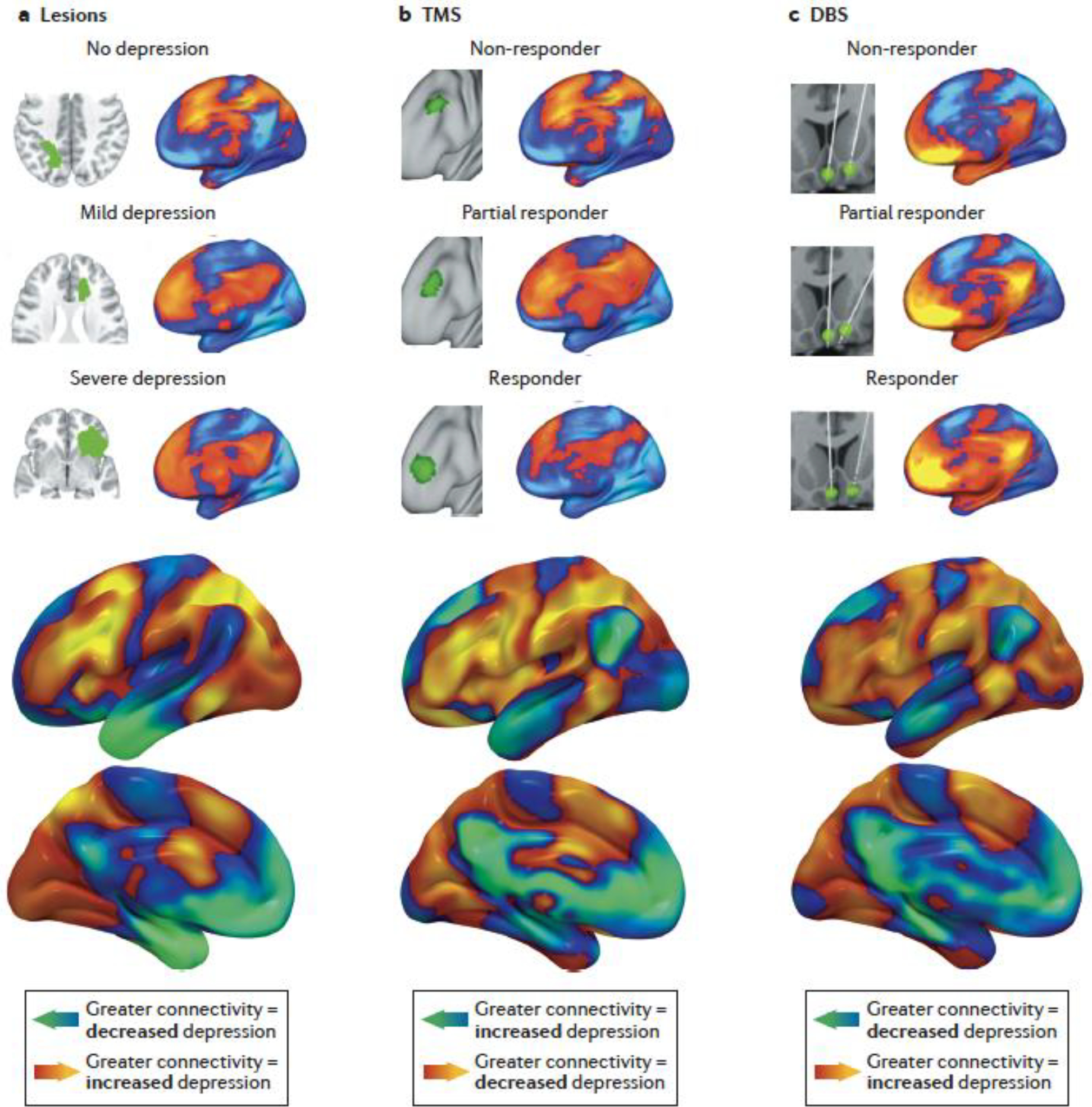
Mapping human brain function is a long-standing goal of neuroscience that promises to inform the development of new treatments for brain disorders. Early maps of human brain function were based on locations of brain damage or brain stimulation that caused a functional change. Over time, this approach was largely replaced by technologies such as functional neuroimaging, which identify brain regions in which activity is correlated with behaviours or symptoms. Despite their advantages, these technologies reveal correlations, not causation. This creates challenges for interpreting the data generated from these tools and using them to develop treatments for brain disorders. A return to causal mapping of human brain function based on brain lesions and brain stimulation is underway. New approaches can combine these causal sources of information with modern neuroimaging and electrophysiology techniques to gain new insights into the functions of specific brain areas. In this Review, we provide a definition of causality for translational research, propose a continuum along which to assess the relative strength of causal information from human brain mapping studies and discuss recent advances in causal brain mapping and their relevance for developing treatments.
© 2022. Springer Nature Limited.
Figures


References
-
- Fox MD & Raichle ME Spontaneous fluctuations in brain activity observed with functional magnetic resonance imaging. Nature reviews neuroscience 8, 700–711 (2007). - PubMed
-
- Raichle ME A brief history of human brain mapping. Trends in neurosciences 32, 118–126 (2009). - PubMed
-
- Gusnard DA & Raichle ME Searching for a baseline: functional imaging and the resting human brain. Nature reviews neuroscience 2, 685–694 (2001). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
