

Mandibular Movements are a Reliable Noninvasive Alternative to Esophageal Pressure for Measuring Respiratory Effort in Patients with Sleep Apnea Syndrome
- PMID: 35444480
- PMCID: PMC9013709
- DOI: 10.2147/NSS.S346229
Mandibular Movements are a Reliable Noninvasive Alternative to Esophageal Pressure for Measuring Respiratory Effort in Patients with Sleep Apnea Syndrome
Abstract
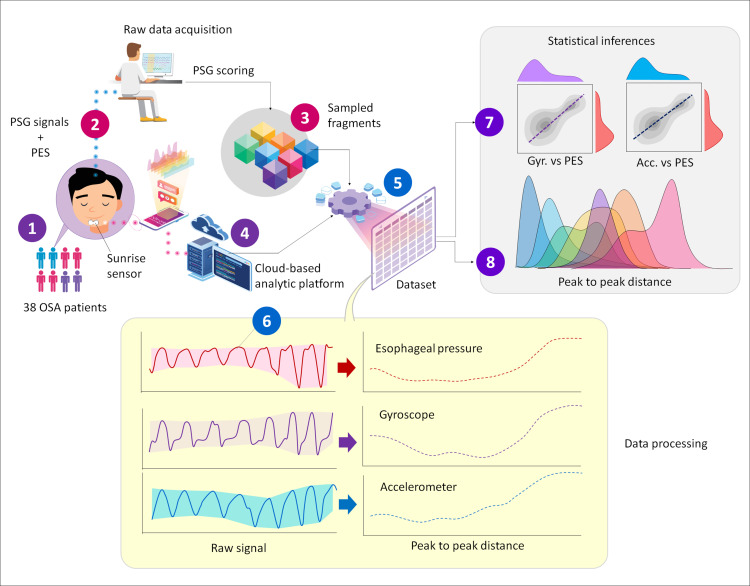
Purpose: Differentiation between obstructive and central apneas and hypopneas requires quantitative measurement of respiratory effort (RE) using esophageal pressure (PES), which is rarely implemented. This study investigated whether the sleep mandibular movements (MM) signal recorded with a tri-axial gyroscopic chin sensor (Sunrise, Namur, Belgium) is a reliable surrogate of PES in patients with suspected obstructive sleep apnea (OSA).
Patients and methods: In-laboratory polysomnography (PSG) with PES and concurrent MM monitoring was performed. PSGs were scored manually using AASM 2012 rules. Data blocks (n=8042) were randomly sampled during normal breathing (NB), obstructive or central apnea/hypopnea (OA/OH/CA/CH), respiratory effort-related arousal (RERA), and mixed apnea (MxA). Analyses were evaluation of the similarity and linear correlation between PES and MM using the longest common subsequence (LCSS) algorithm and Pearson's coefficient; description of signal amplitudes; estimation of the marginal effect for crossing from NB to a respiratory disturbance for a given change in MM signal using a mixed linear-regression.
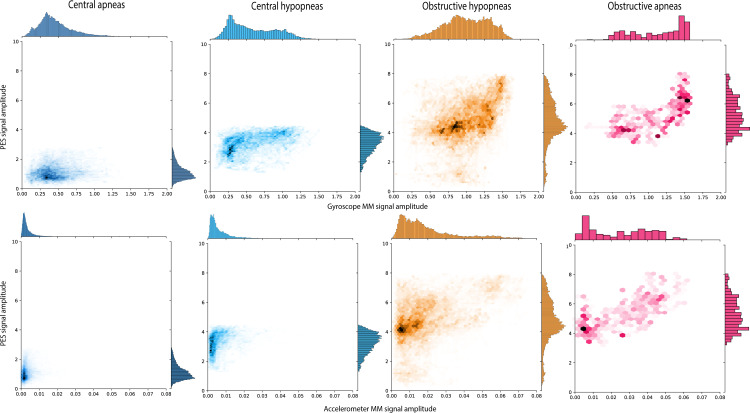
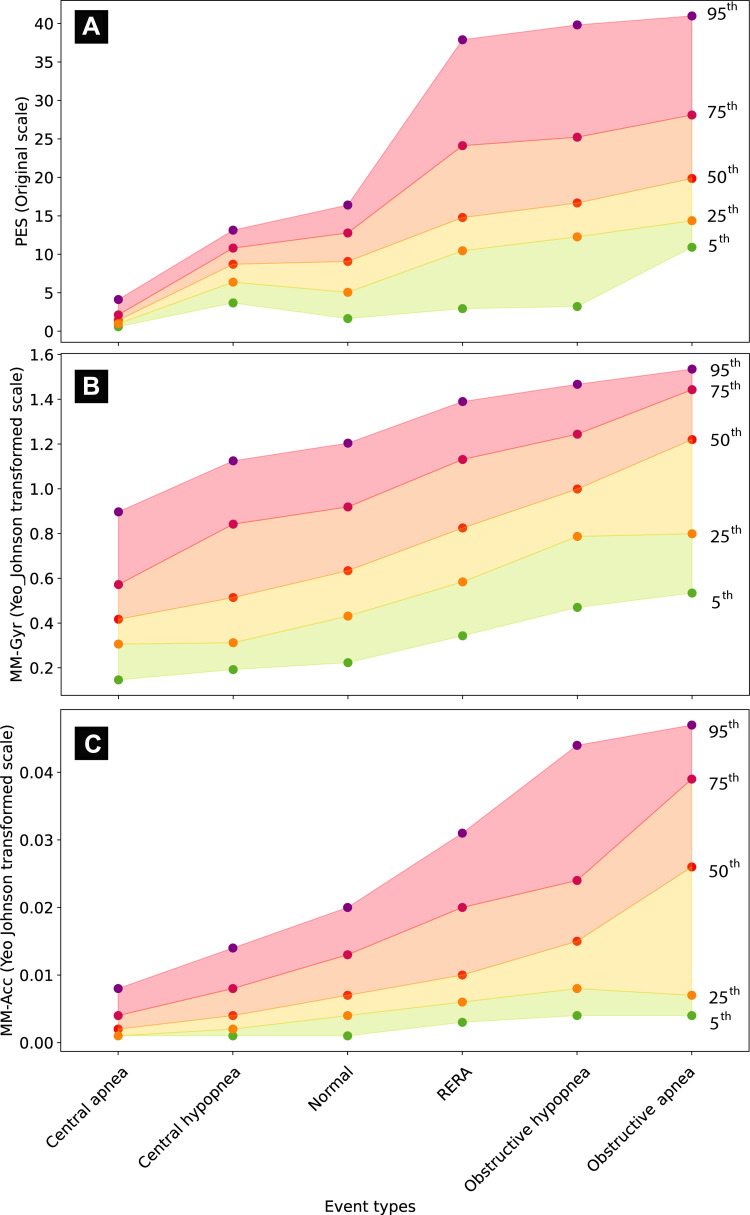
Results: Participants (n=38) had mild to severe OSA (median AH index 28.9/h; median arousal index 23.2/h). MM showed a high level of synchronization with concurrent PES signals. Distribution of MM amplitude differed significantly between event types: median (95% confidence interval) values of 0.60 (0.16-2.43) for CA, 0.83 (0.23-4.71) for CH, 1.93 (0.46-12.43) for MxA, 3.23 (0.72-18.09) for OH, and 6.42 (0.88-26.81) for OA. Mixed regression indicated that crossing from NB to central events would decrease MM signal amplitude by -1.23 (CH) and -2.04 (CA) units, while obstructive events would increase MM amplitude by +3.27 (OH) and +6.79 (OA) units (all p<10-6).
Conclusion: In OSA patients, MM signals facilitated the measurement of specific levels of RE associated with obstructive, central or mixed apneas and/or hypopneas. A high degree of similarity was observed with the PES gold-standard signal.
Keywords: esophageal pressure; mandibular movements; obstructive sleep apnea; respiratory effort.
© 2022 Pepin et al.
Conflict of interest statement
J-L.P. reports being a scientific advisor to Sunrise; receiving grants and/or personal fees from ResMed, Philips, Fisher & Paykel, Sefam, AstraZeneca, AGIR à dom, Elevie, VitalAire, Boehringer Ingelheim, Jazz Pharmaceuticals, Night Balance, and Itamar Medical Ltd; and receiving research support for clinical studies from Mutualia and Air Liquide Foundation. N-N.L-Dong is an employee of Sunrise. J-B.M. reports being a non-remunerated scientific advisor to Sunrise and being an investigator in pharmacy trials for Jazz Pharmaceuticals, Theranexus and Desitin. RT reports grants from Resmed, board and lecture fees from Jazz Pharm and Bioprojet, outside the submitted work. AM reports income related to medical education from Livanova, Equillium, Jazz, Sunrise, Corvus; ResMed provided a philanthropic donation to UCSD. All other authors have no conflicts of interest to declare in this work.
Figures

References
-
- Berry RB, Budhiraja R, Gottlieb DJ, et al. Rules for scoring respiratory events in sleep: update of the 2007 AASM manual for the scoring of sleep and associated events. Deliberations of the sleep apnea definitions task force of the American Academy of Sleep Medicine. J Clin Sleep Med. 2012;8(5):597–619. doi: 10.5664/jcsm.2172 - DOI - PMC - PubMed
