

The Importance of Magnetic Resonance in Detection of Cortical Dysplasia
- PMID: 35444831
- PMCID: PMC8987480
- DOI: 10.12865/CHSJ.47.04.16
The Importance of Magnetic Resonance in Detection of Cortical Dysplasia
Abstract
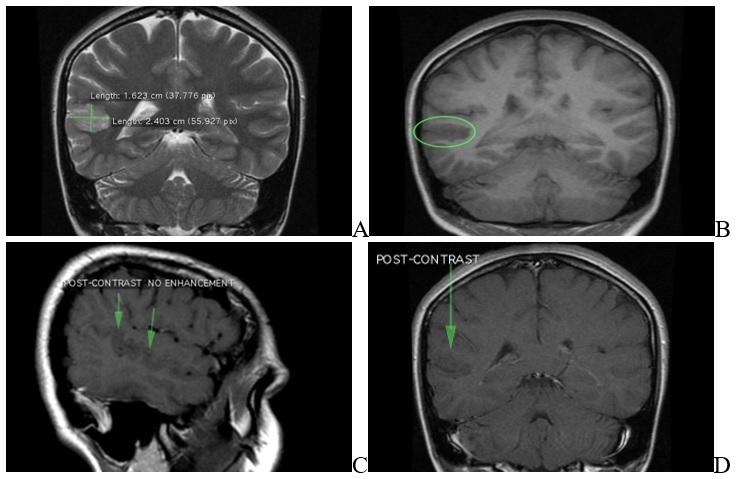
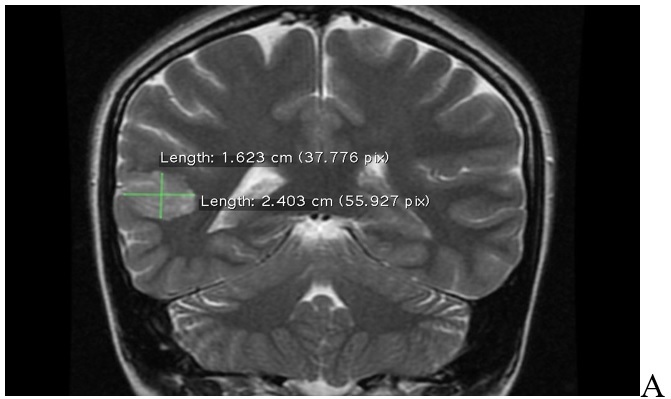
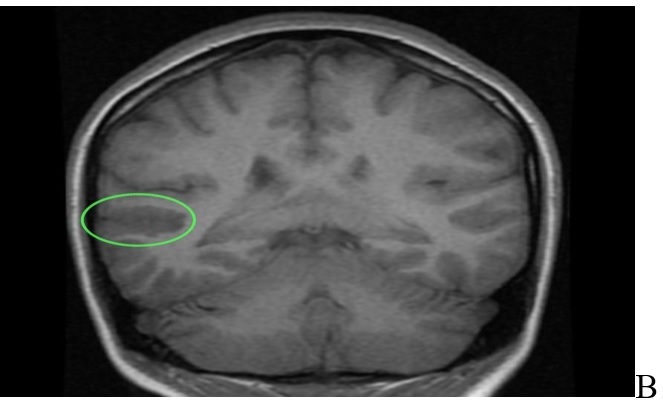
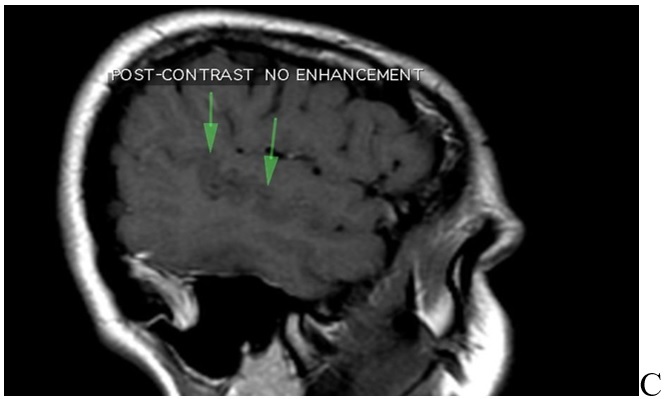
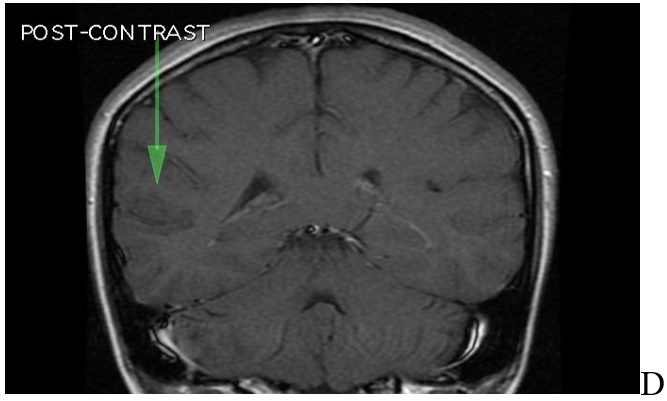
Focal cortical dysplasia is a malformation of cortical development in which there are abnormalities with cortical lamination, neuronal maturation, and neuronal differentiation. It is the most common cause of medically refractory epilepsy in the pediatric population and the second/third most common etiology of medically intractable seizures in adults. Herein, we present the case of 23-years-old female patient, presenting with loss of consciousness, and convulsions. A MRI revealed a 5mm cortical thickening on either side of the posterior aspect of the right superior temporal gyrus without transmantle extension towards ventricle. This abnormal area is measured about 24x16mm and there was no evidence for mesial temporal sclerosis. Both hippocampi are normal is size, morphology and signal. These features are consistent with cortical dysplasia type 1. This case report emphasizes the importance of MRI in the detection of FCD. MRI can show no abnormalities in type 1 FCD, but when the changes are apparent, they are on the temporal lobe, and seizures presents most commonly in adults.
Keywords: Focal cortical dysplasia; cortical development; hippocampus; neuronal maturation.
Copyright © 2014, Medical University Publishing House Craiova.
Conflict of interest statement
None to declare.
Figures
References
-
- Blümcke I, Thom M, Aronica E, Armstrong DD, Vinters HV, Palmini A, Jacques TS, Avanzini G, Barkovich AJ, Battaglia G, Becker A, Cepeda C, Cendes F, Colombo N, Crino P, Cross JH, Delalande O, Dubeau F, Duncan J, Guerrini R, Kahane P, Mathern G, Najm I, Ozkara C, Raybaud C, Represa A, Roper SN, Salamon N, Schulze-Bonhage A, Tassi L, Vezzani A, Spreafico R. The clinicopathologic spectrum of focal cortical dysplasias: a consensus classification proposed by an ad hoc Task Force of the ILAE Diagnostic Methods Commission. Epilepsia. 2011;52(1):158–174. - PMC - PubMed
-
- Mountcastle VB. The columnar organization of the neocortex. Brain. 1997;120(Pt 4):701–722. - PubMed
-
- Sarnat HB, Flores-Sarnat L. Radial microcolumnar cortical architecture: maturational arrest or cortical dysplasia. Pediatr Neurol. 2013;48(4):259–270. - PubMed
-
- Blümcke I, Sarnat HB, Coras R. Surgical neuropathology of focal epilepsies: textbook and atlas. Montrouge: John Libbey Eurotext. 2015
-
- Kobow K, Ziemann M, Kaipananickal H, Khurana I, Mühlebner A, Feucht M, Hainfellner JA, Czech T, Aronica E, Pieper T, Holthausen H, Kudernatsch M, Hamer H, Kasper BS, Rössler K, Conti V, Guerrini R, Coras R, Blümcke I, El-Osta A, Kaspi A. Genomic DNA methylation distinguishes subtypes of human focal cortical dysplasia. Epilepsia. 2019;60(6):1091–1103. - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources