

Connective tissue disease-related interstitial lung disease (CTD-ILD) and interstitial lung abnormality (ILA): Evolving concept of CT findings, pathology and management
- PMID: 35445144
- PMCID: PMC9014394
- DOI: 10.1016/j.ejro.2022.100419
Connective tissue disease-related interstitial lung disease (CTD-ILD) and interstitial lung abnormality (ILA): Evolving concept of CT findings, pathology and management
Abstract
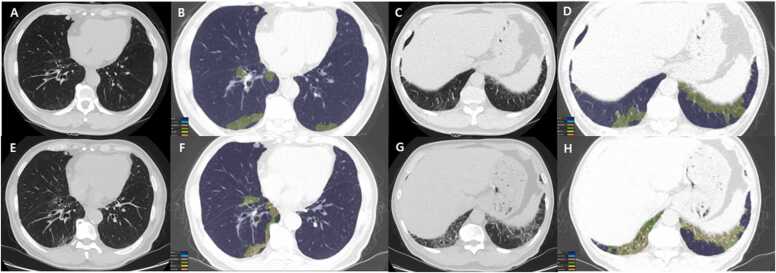
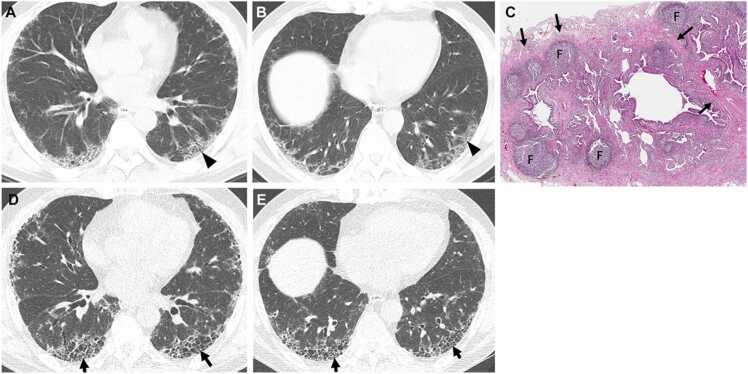
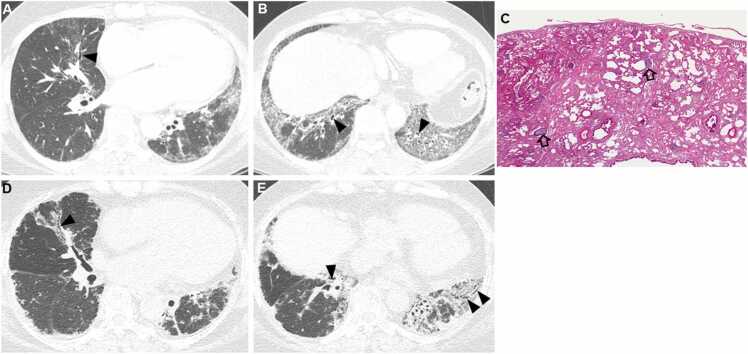
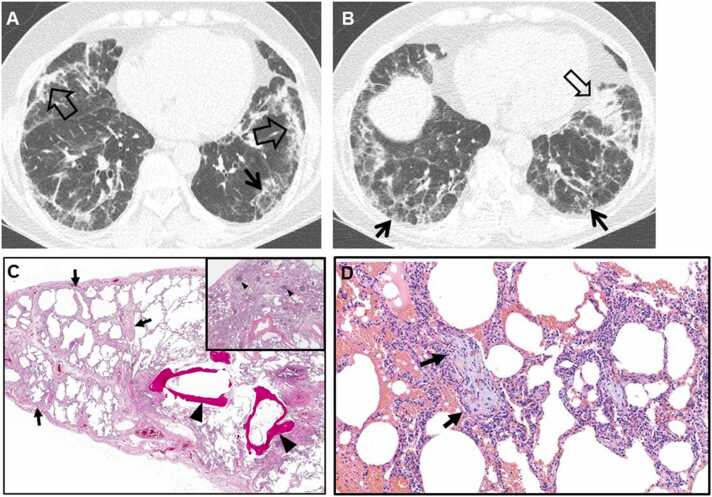
Connective tissue diseases (CTDs) demonstrating features of interstitial lung disease (ILD) include systemic lupus erythematosus (SLE), rheumatoid arthritis (RA), systemic sclerosis (SSc), dermatomyositis (DM) and polymyositis (PM), ankylosing spondylitis (AS), Sjogren syndrome (SS), and mixed connective tissue disease (MCTD). On histopathology of lung biopsy in CTD-related ILDs (CTD-ILDs), multi-compartment involvement is an important clue, and when present, should bring CTD to the top of the list of etiologic differential diagnoses. Diverse histologic patterns including nonspecific interstitial pneumonia (NSIP), usual interstitial pneumonia (UIP), organizing pneumonia, apical fibrosis, diffuse alveolar damage, and lymphoid interstitial pneumonia can be seen on histology in patients with CTD-ILDs. Although proportions of ILDs vary, the NSIP pattern accounts for a large proportion, especially in SSc, DM and/or PM and MCTD, followed by the UIP pattern. In RA patients, interstitial lung abnormality (ILA) is reported to occur in approximately 20-60% of individuals of which 35-45% will have progression of the CT abnormality. Subpleural distribution and greater baseline ILA involvement are risk factors associated with disease progression. Asymptomatic CTD-ILDs or ILA patients with normal lung function and without evidence of disease progression can be followed without treatment. Immunosuppressive or antifibrotic agents for symptomatic and/or fibrosing CTD-ILDs can be used in patients who require treatment.
Keywords: CTD, Connective tissue disease; CTD-ILD, Connective tissue disease-related interstitial lung disease; Connective tissue disease; DM, Dermatomyositis; IIP, Idiopathic interstitial pneumonia; ILA, Interstitial lung abnormality; ILD, Interstitial lung disease; IPAF, Interstitial pneumonitis with autoimmune features; IPF, Idiopathic pulmonary fibrosis; Interstitial lung abnormality; Interstitial lung disease; LIP, Lymphoid interstitial pneumonia; MCTD, Mixed connective tissue disease; NSIP, Nonspecific interstitial pneumonia; OP, Organizing pneumonia; PM, Polymyositis; RA, Rheumatoid arthritis; SLE, Systemic lupus erythematosus; SS, Sjogren’s syndrome; SSc, Systemic sclerosis; UCTD, Undifferentiated connective tissue disease; UIP, Usual interstitial pneumonia.
© 2022 The Authors.
Figures
References
-
- American Thoracic Society/European Respiratory Society International Multidisciplinary Consensus Classification of the Idiopathic Interstitial Pneumonias. This joint statement of the American Thoracic Society (ATS), and the European Respiratory Society (ERS) was adopted by the ATS board of directors, June 2001 and by the ERS Executive Committee, June 2001, Am J Respir Crit Care Med 165 (2002) 277–304. https://doi.org/10.1164/ajrccm.165.2.ats01. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
