

Prevalence and Cost of Care Cascades Following Low-Value Preoperative Electrocardiogram and Chest Radiograph Within the Veterans Health Administration
- PMID: 35445352
- PMCID: PMC9905526
- DOI: 10.1007/s11606-022-07561-x
Prevalence and Cost of Care Cascades Following Low-Value Preoperative Electrocardiogram and Chest Radiograph Within the Veterans Health Administration
Abstract
Background: Low-value care cascades, defined as the receipt of downstream health services potentially related to a low-value service, can result in harm to patients and wasteful healthcare spending, yet have not been characterized within the Veterans Health Administration (VHA).
Objective: To examine if the receipt of low-value preoperative testing is associated with greater utilization and costs of potentially related downstream health services in Veterans undergoing low or intermediate-risk surgery.
Design: Retrospective cohort study using VHA administrative data from fiscal years 2017-2018 comparing Veterans who underwent low-value preoperative electrocardiogram (EKG) or chest radiograph (CXR) with those who did not.
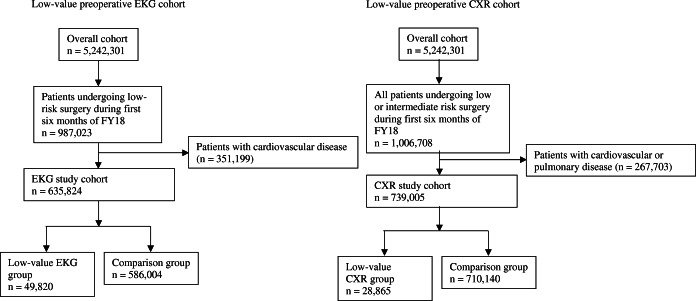
Participants: National cohort of Veterans at low risk of cardiopulmonary disease undergoing low- or intermediate-risk surgery.
Main measures: Difference in rate of receipt and attributed cost of potential cascade services in Veterans who underwent low-value preoperative testing compared to those who did not KEY RESULTS: Among 635,824 Veterans undergoing low-risk procedures, 7.8% underwent preoperative EKG. Veterans who underwent a preoperative EKG experienced an additional 52.4 (95% CI 47.7-57.2) cascade services per 100 Veterans, resulting in $138.28 (95% CI 126.19-150.37) per Veteran in excess costs. Among 739,005 Veterans undergoing low- or intermediate-risk surgery, 3.9% underwent preoperative CXR. These Veterans experienced an additional 61.9 (95% CI 57.8-66.1) cascade services per 100 Veterans, resulting in $152.08 (95% CI $146.66-157.51) per Veteran in excess costs. For both cohorts, care cascades consisted largely of repeat tests, follow-up imaging, and follow-up visits, with low rates invasive services.
Conclusions: Among a national cohort of Veterans undergoing low- or intermediate-risk surgeries, low-value care cascades following two routine low-value preoperative tests are common, resulting in greater unnecessary care and costs beyond the initial low-value service. These findings may guide de-implementation policies within VHA and other integrated healthcare systems that target those services whose downstream effects are most prevalent and costly.
Keywords: Veterans Health Administration; care cascades; low-value care; preoperative testing.
© 2022. The Author(s), under exclusive licence to Society of General Internal Medicine.
Conflict of interest statement
Aaron Schwartz reports receiving personal fees from the Lown Institute, CVS Health, and the Medicare Payment Advisory Commission for prior research consulting outside the scope of the submitted work.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
