

Effect of dapagliflozin on kidney and cardiovascular outcomes by baseline KDIGO risk categories: a post hoc analysis of the DAPA-CKD trial
- PMID: 35445820
- PMCID: PMC9174107
- DOI: 10.1007/s00125-022-05694-6
Effect of dapagliflozin on kidney and cardiovascular outcomes by baseline KDIGO risk categories: a post hoc analysis of the DAPA-CKD trial
Abstract
Aims/hypothesis: In the Dapagliflozin and Prevention of Adverse Outcomes in Chronic Kidney Disease (DAPA-CKD) trial, dapagliflozin reduced the risks of progressive kidney disease, hospitalised heart failure or cardiovascular death, and death from all causes in patients with chronic kidney disease (CKD) with or without type 2 diabetes. Patients with more severe CKD are at higher risk of kidney failure, cardiovascular events and all-cause mortality. In this post hoc analysis, we assessed the efficacy and safety of dapagliflozin according to baseline Kidney Disease Improving Global Outcomes (KDIGO) risk categories.
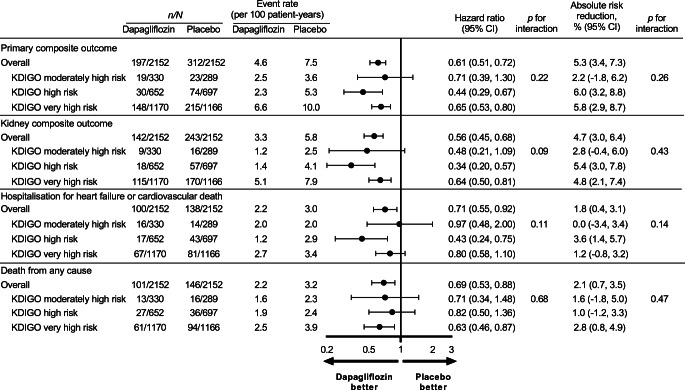
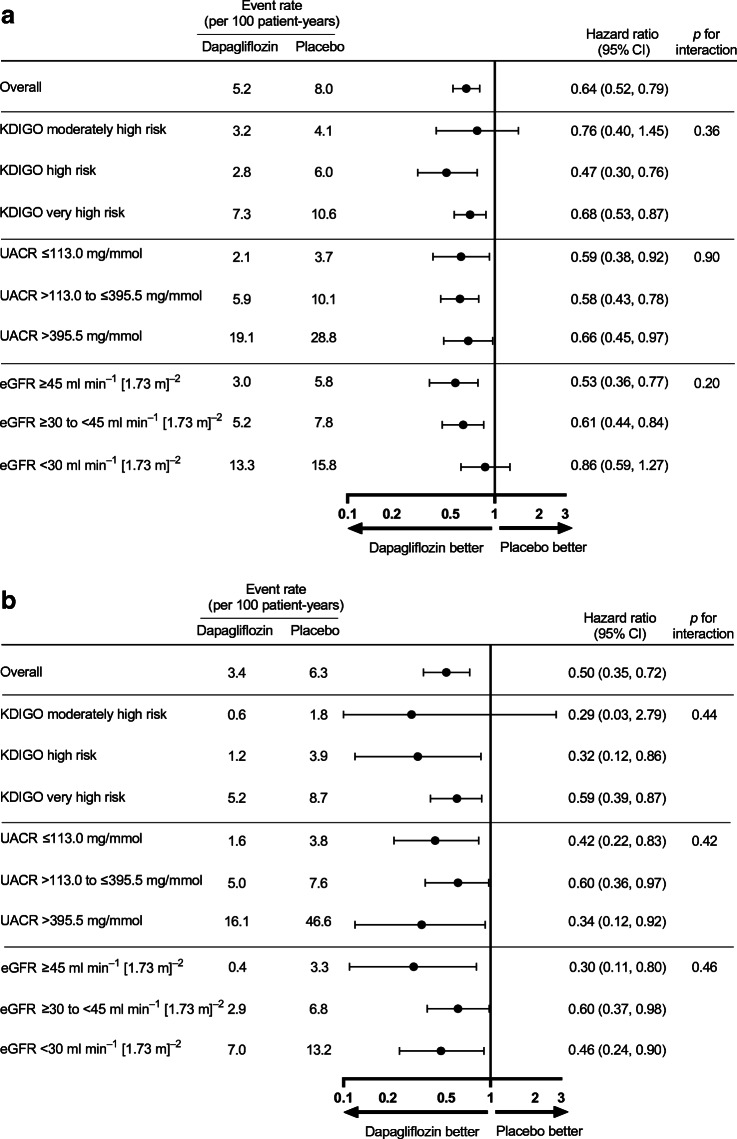
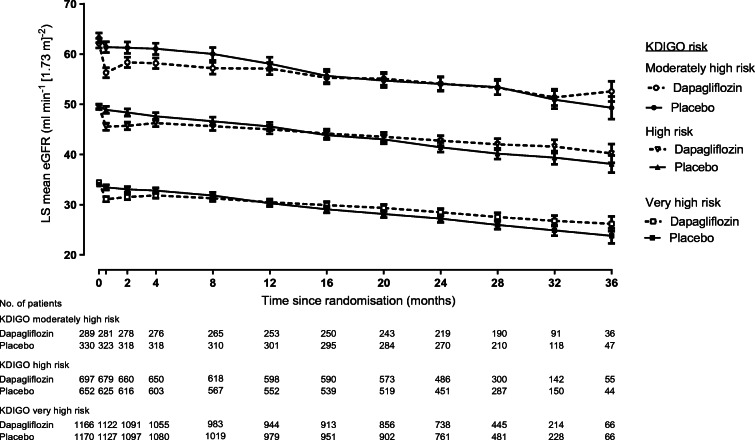
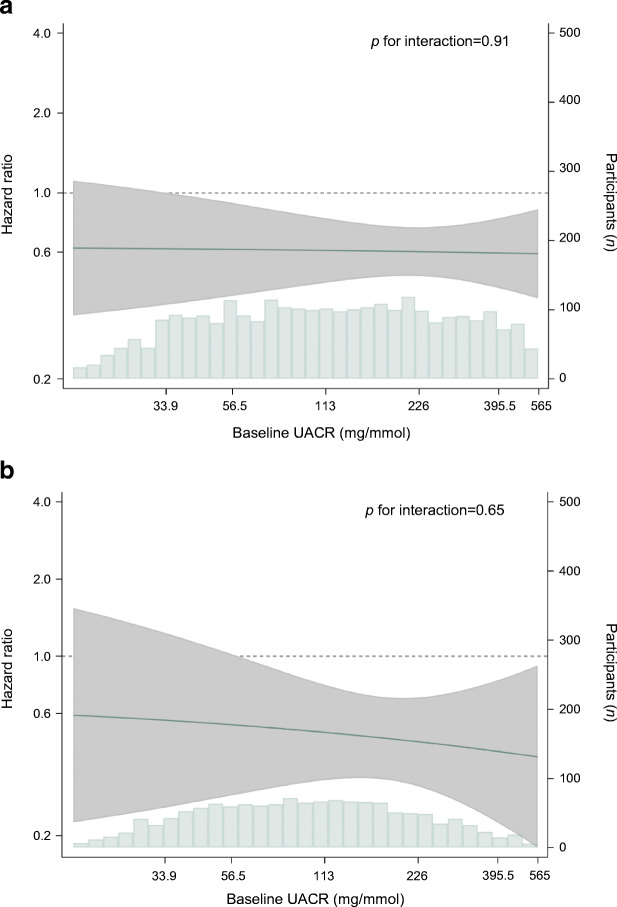
Methods: DAPA-CKD was a double-blind, placebo-controlled trial that randomised patients with an eGFR of 25-75 ml min-1 [1.73 m]-2 and urinary albumin/creatinine ratio (UACR) of ≥22.6 and <565.0 mg/mmol (200-5000 mg/g) to dapagliflozin 10 mg/day or placebo. The primary endpoint was a composite of ≥50% reduction in eGFR, end-stage kidney disease (ESKD), and death from a kidney or cardiovascular cause. Secondary endpoints included a kidney composite (≥50% reduction in eGFR, ESKD and death from a kidney cause), a cardiovascular composite (heart failure hospitalisation or cardiovascular death), and death from all causes. We used Cox proportional hazards regression analyses to assess relative and absolute effects of dapagliflozin across KDIGO risk categories.
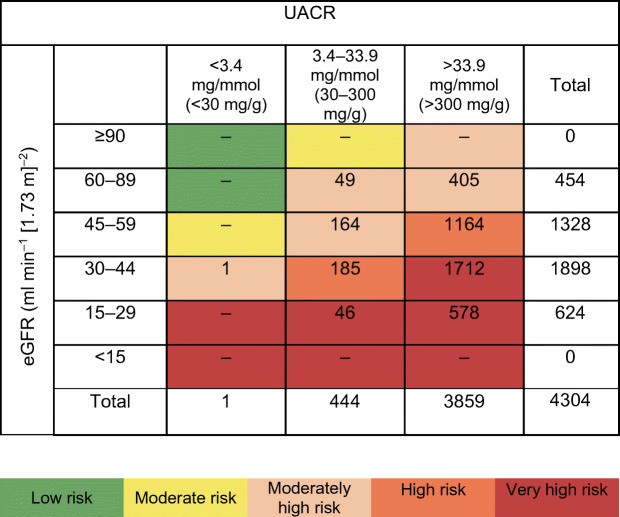
Results: Of the 4304 participants in the DAPA-CKD study, 619 (14.4%) were moderately high risk, 1349 (31.3%) were high risk and 2336 (54.3%) were very high risk when categorised by KDIGO risk categories at baseline. Dapagliflozin reduced the hazard of the primary composite (HR 0.61; 95% CI 0.51, 0.72) and secondary endpoints consistently across KDIGO risk categories (all p for interaction >0.09). Absolute risk reductions for the primary outcome were also consistent irrespective of KDIGO risk category (p for interaction 0.26). Analysing patients with and without type 2 diabetes separately, the relative risk reduction with dapagliflozin in terms of the primary outcome was consistent across subgroups of KDIGO risk categories. The relative frequencies of adverse events and serious adverse events were also similar across KDIGO risk categories.
Conclusion/interpretations: The consistent benefits of dapagliflozin on kidney and cardiovascular outcomes across KDIGO risk categories indicate that dapagliflozin is efficacious and safe across a wide spectrum of kidney disease severity.
Trial registration: ClinicalTrials.gov NCT03036150.
Funding: The study was funded by AstraZeneca.
Keywords: Albuminuria; Dapagliflozin; KDIGO risk categories; Kidney outcome; SGLT2 inhibitor; eGFR.
© 2022. The Author(s).
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
