

Prediction of long-term dependence on vitamin D analogues following total thyroidectomy for Graves' disease
- PMID: 35446722
- PMCID: PMC9889183
- DOI: 10.1308/rcsann.2022.0007
Prediction of long-term dependence on vitamin D analogues following total thyroidectomy for Graves' disease
Abstract
Introduction: This study aimed to identify patients at risk of long-term hypocalcaemia following total thyroidectomy for Graves' disease, and to determine the thresholds of postoperative day 1 serum calcium and parathyroid hormone (PTH) at which long-term activated vitamin D treatment can be safely excluded.
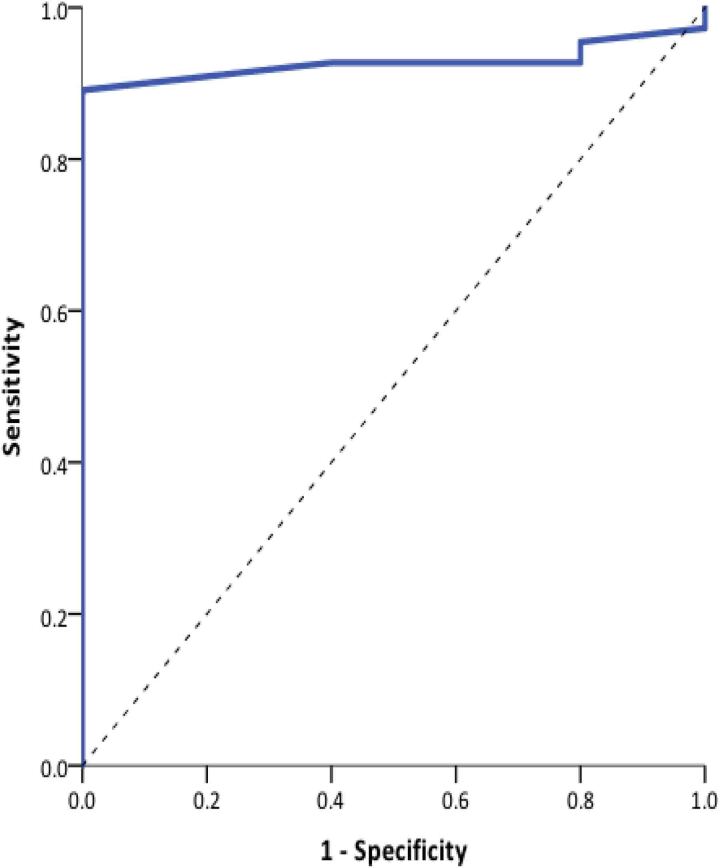
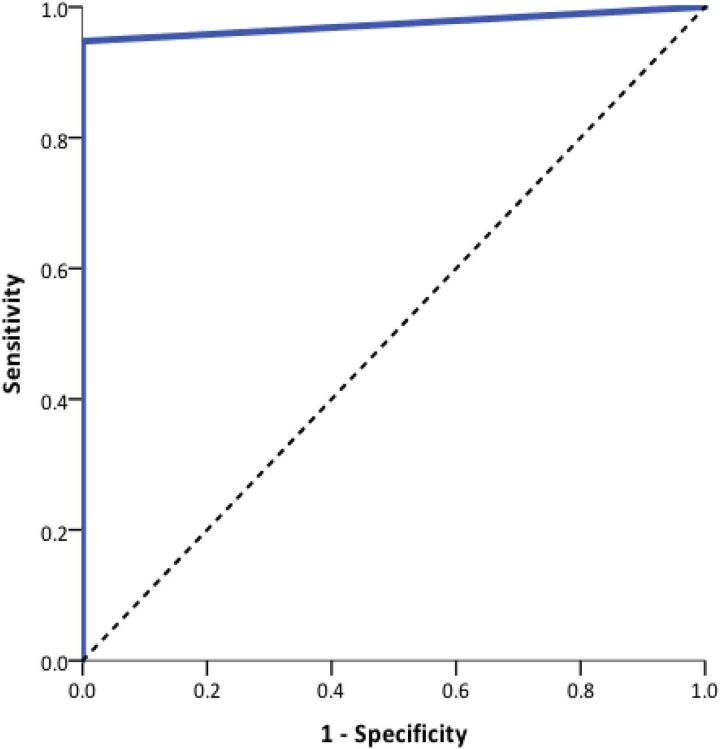
Methods: This study was a retrospective analysis of 115 consecutive patients undergoing total thyroidectomy for Graves' disease at a university referral centre between 2010 and 2018. Outcome measures were the day 1 postoperative adjusted calcium and PTH results, and vitamin D analogue need at 6 months postoperatively. Logistic receiver operating curves were used to identify optimal cut-off values for adjusted serum calcium and serum PTH, and sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated.
Results: Temporary hypocalcaemia was observed in 20.9% of patients (mean day 1 serum adjusted calcium 2.2±0.14mmol/l and PTH 4.15±2.42pmol/l). Long-term (>6 months) activated vitamin D analogue therapy was required in five patients (4.3%), four of whom had normal serum PTH and one with undetectable PTH at 6 weeks post surgery. No patient with a day 1 postoperative calcium >2.05mmol/l and detectable PTH required vitamin D supplementation at 6 months post surgery (100% sensitivity, PPV 50%, NPV 100%).
Conclusions: The biochemical postoperative day 1 thresholds identified in this paper have a 100% NPV in the identification of patients who are likely to require either no or only temporary activated vitamin D supplementation. We were able to identify all patients requiring activated vitamin D supplementation 6 months postoperatively from the day 1 postoperative serum calcium and PTH values, while excluding those that may only need temporary calcium supplementation. These threshold levels could be used for targeted follow-up and management of this subset of patients most at risk of long-term hypocalcaemia.
Keywords: Calcium; Graves’ disease; Hypoparathyroidism; Parathyroid hormone; Total thyroidectomy.
Figures
References
-
- Burch HB, Cooper DS. Management of graves disease a review. JAMA 2015; 314: 2544–2554. - PubMed
-
- El Malki HO, Abouqal R. Systematic review and meta-analysis of predictors of post-thyroidectomy hypocalcaemia. Br J Surg 2014; 101: 883. - PubMed
-
- Almquist M, Ivarsson K, Nordenström E, Bergenfelz A. Mortality in patients with permanent hypoparathyroidism after total thyroidectomy. Br J Surg 2018; 105: 1313–1318. - PubMed
-
- Chadwick D, Kinsman R, Walton P, editors. British Association of Endocrine and Thyroid Surgeons. Fifth National Audit Report. 5th ed. Henley-on-Thames: Dendrite Clinical Systems Ltd; 2017.
-
- Agha R, Abdall-Razak A, Crossley Eet al. STROCSS 2019 guideline: strengthening the reporting of cohort studies in surgery. Int J Surg 2019; 72: 156–165. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources