

The mTOR inhibitor Rapamycin protects from premature cellular senescence early after experimental kidney transplantation
- PMID: 35446876
- PMCID: PMC9022825
- DOI: 10.1371/journal.pone.0266319
The mTOR inhibitor Rapamycin protects from premature cellular senescence early after experimental kidney transplantation
Abstract
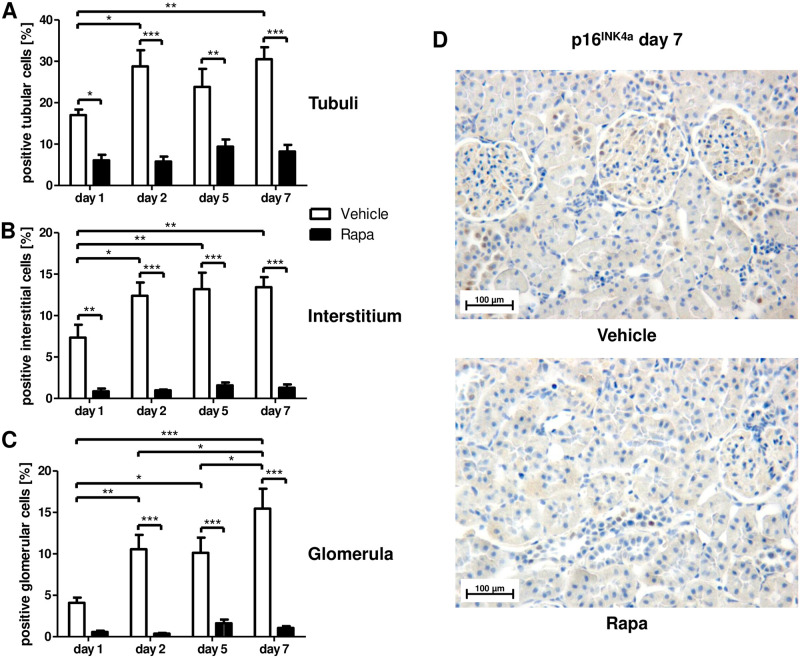
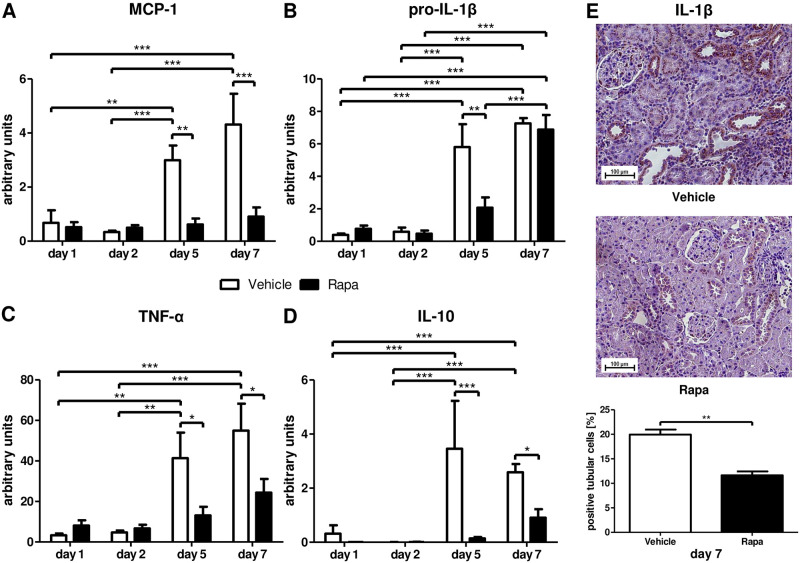
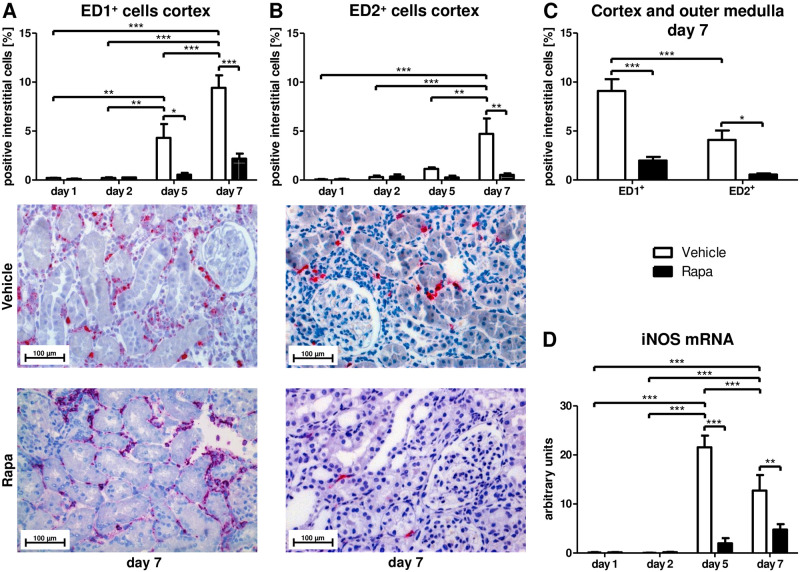
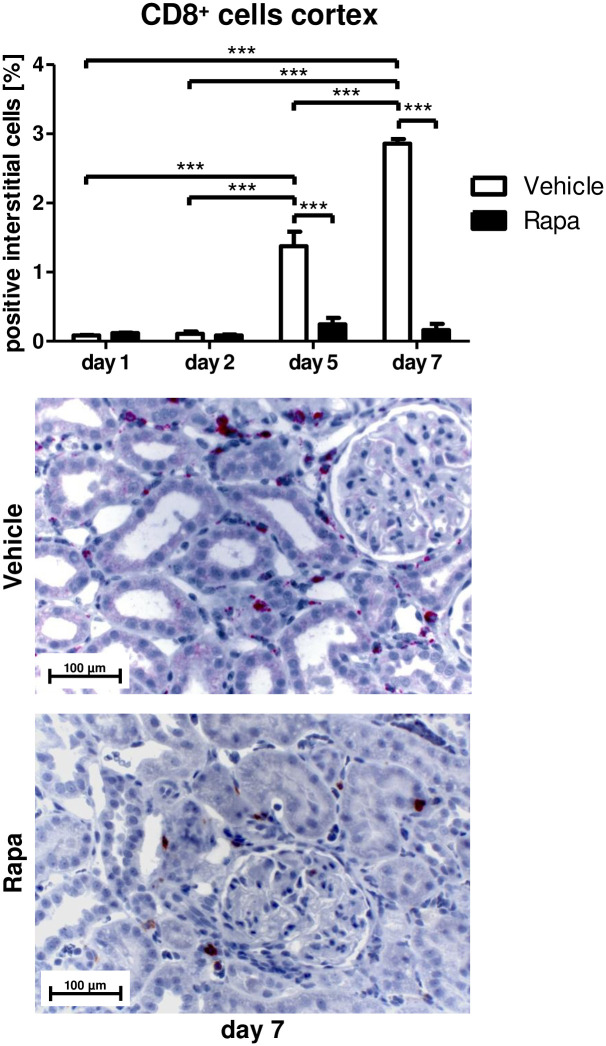
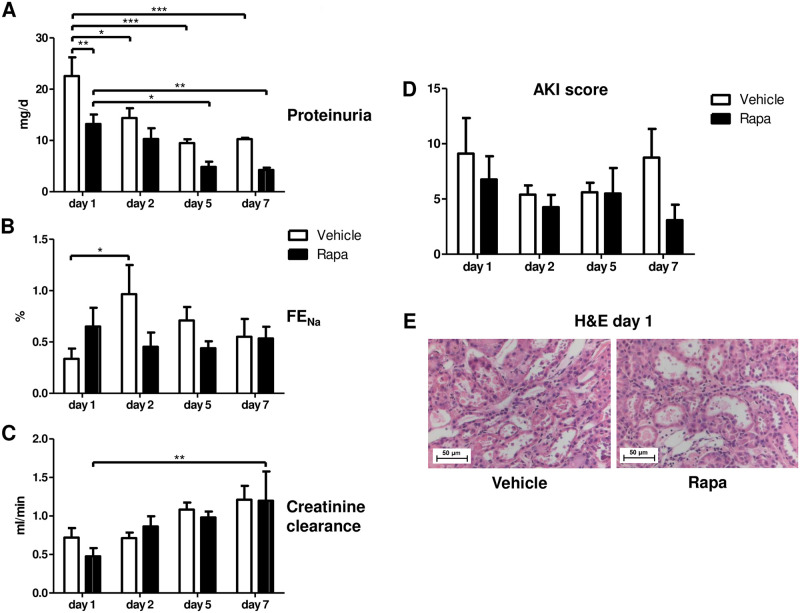
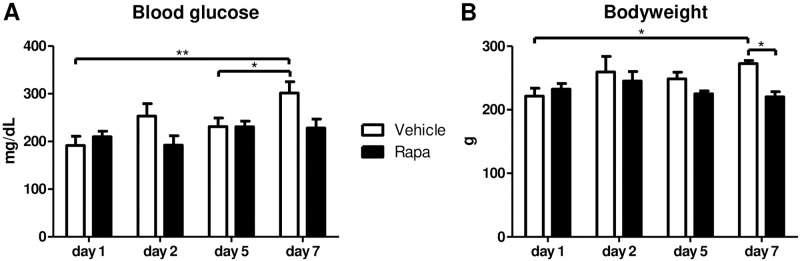
Interstitial fibrosis and tubular atrophy, a major cause of kidney allograft dysfunction, has been linked to premature cellular senescence. The mTOR inhibitor Rapamycin protects from senescence in experimental models, but its antiproliferative properties have raised concern early after transplantation particularly at higher doses. Its effect on senescence has not been studied in kidney transplantation, yet. Rapamycin was applied to a rat kidney transplantation model (3 mg/kg bodyweight loading dose, 1.5 mg/kg bodyweight daily dose) for 7 days. Low Rapamycin trough levels (2.1-6.8 ng/mL) prevented the accumulation of p16INK4a positive cells in tubules, interstitium, and glomerula. Expression of the cytokines MCP-1, IL-1β, and TNF-α, defining the proinflammatory senescence-associated secretory phenotype, was abrogated. Infiltration with monocytes/macrophages and CD8+ T-lymphocytes was reduced and tubular function was preserved by Rapamycin. Inhibition of mTOR was not associated with impaired structural recovery, higher glucose levels, or weight loss. mTOR inhibition with low-dose Rapamycin in the immediate posttransplant period protected from premature cellular senescence without negative effects on structural and functional recovery from preservation/reperfusion damage, glucose homeostasis, and growth in a rat kidney transplantation model. Reduced senescence might maintain the renal regenerative capacity rendering resilience to future injuries resulting in protection from interstitial fibrosis and tubular atrophy.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: Klemens Budde has received research funds and/or honoraria from Abbvie, Alexion, Astellas, Bristol-Myers Squibb, Chiesi, CSL Behring, Fresenius, Hexal, Hookipa Biotech, Merck Sharp & Dohme, Novartis, Otsuka, Pfizer, Roche, Shire, Siemens, Takeda, Veloxis and Vitaeris. All other authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
