

Household Transmission and Symptomology of Severe Acute Respiratory Syndrome Coronavirus 2 Alpha Variant among Children-California and Colorado, 2021
- PMID: 35447121
- PMCID: PMC9015725
- DOI: 10.1016/j.jpeds.2022.04.032
Household Transmission and Symptomology of Severe Acute Respiratory Syndrome Coronavirus 2 Alpha Variant among Children-California and Colorado, 2021
Abstract
Objective: To assess the household secondary infection risk (SIR) of B.1.1.7 (Alpha) and non-Alpha lineages of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) among children.
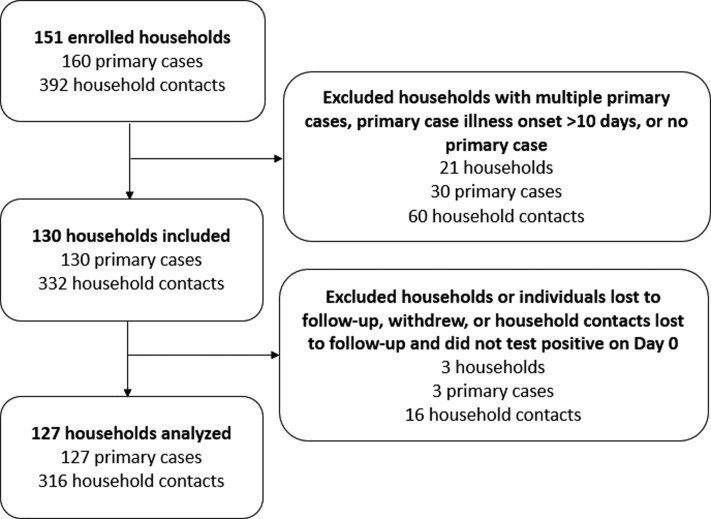
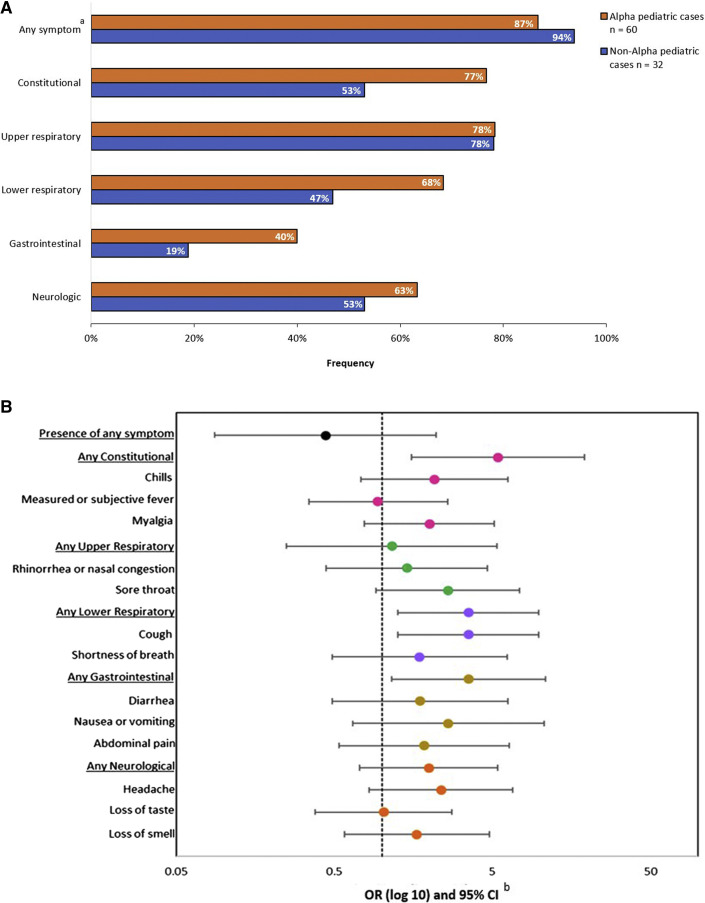
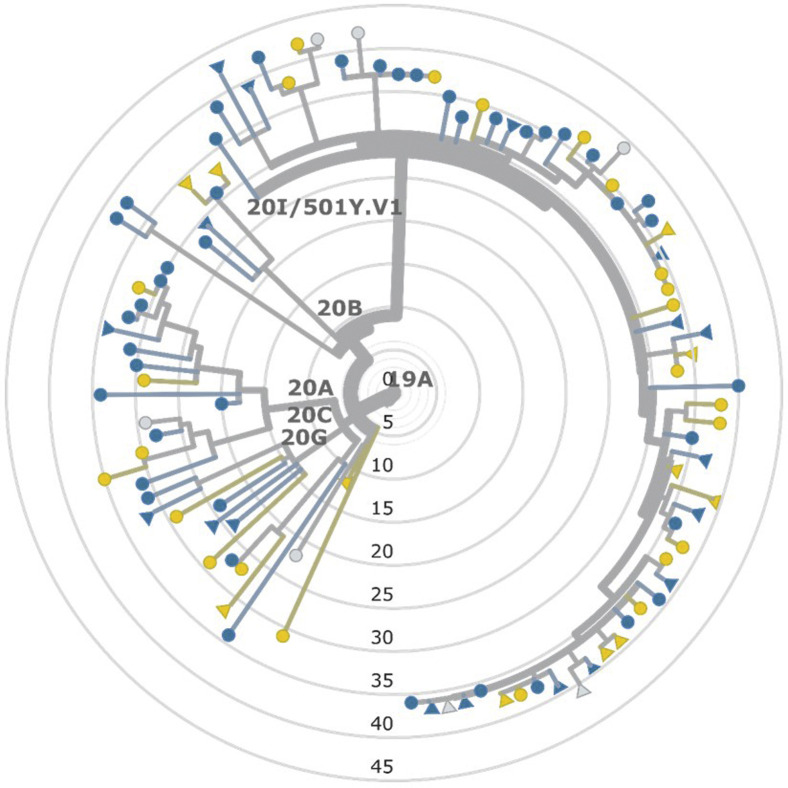
Study design: During January to April 2021, we prospectively followed households with a SARS-CoV-2 infection. We collected questionnaires, serial nasopharyngeal swabs for reverse transcription polymerase chain reaction testing and whole genome sequencing, and serial blood samples for serology testing. We calculated SIRs by primary case age (pediatric vs adult), household contact age, and viral lineage. We evaluated risk factors associated with transmission and described symptom profiles among children.
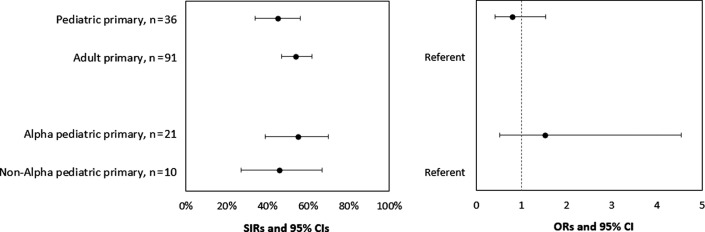
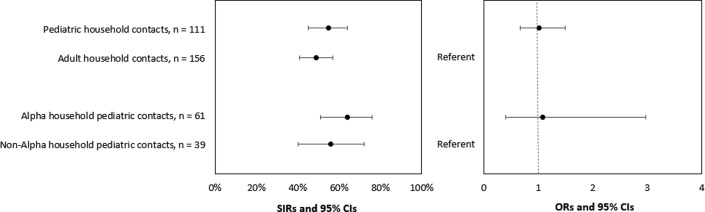
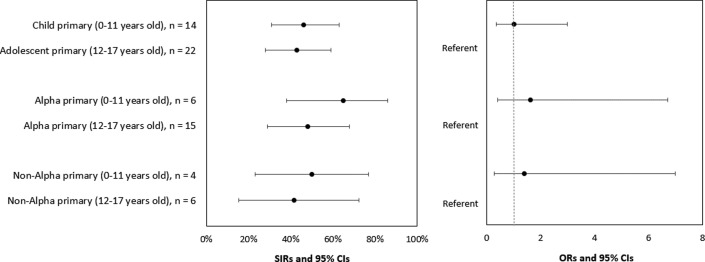
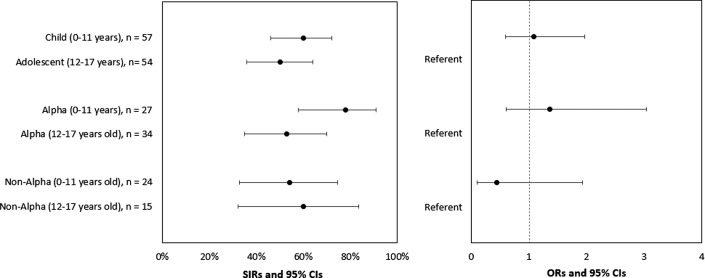
Results: Among 36 households with pediatric primary cases, 21 (58%) had secondary infections. Among 91 households with adult primary cases, 51 (56%) had secondary infections. SIRs among pediatric and adult primary cases were 45% and 54%, respectively (OR, 0.79; 95% CI, 0.41-1.54). SIRs among pediatric primary cases with Alpha and non-Alpha lineage were 55% and 46%, respectively (OR, 1.52; 95% CI, 0.51-4.53). SIRs among pediatric and adult household contacts were 55% and 49%, respectively (OR, 1.01; 95% CI, 0.68-1.50). Among pediatric contacts, no significant differences in the odds of acquiring infection by demographic or household characteristics were observed.
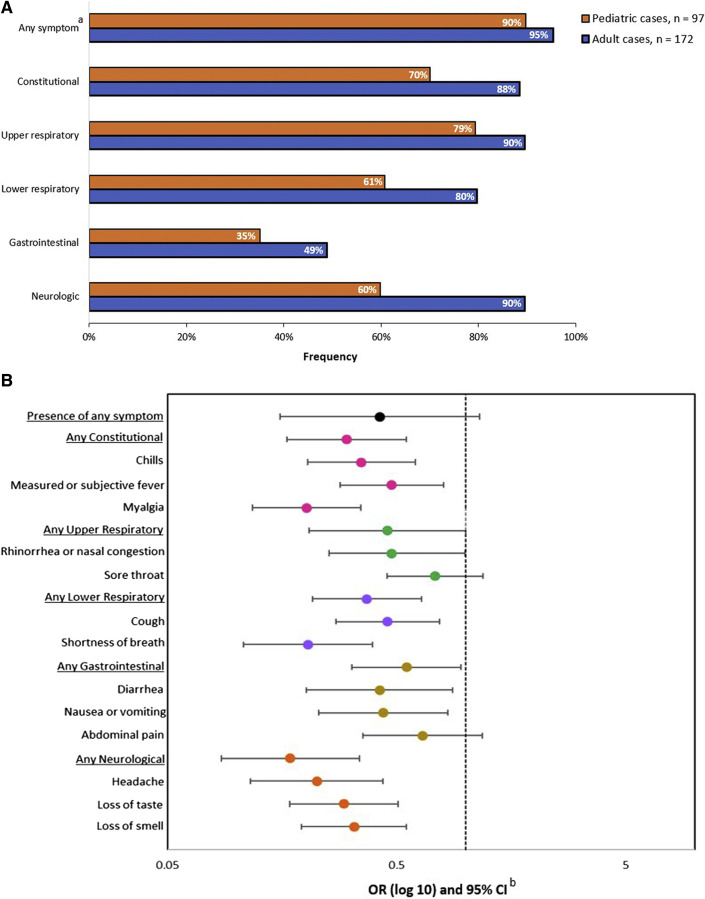
Conclusions: Household transmission of SARS-CoV-2 from children and adult primary cases to household members was frequent. The risk of secondary infection was similar among child and adult household contacts. Among children, household transmission of SARS-CoV-2 and the risk of secondary infection was not influenced by lineage. Continued mitigation strategies (eg, masking, physical distancing, vaccination) are needed to protect at-risk groups regardless of virus lineage circulating in communities.
Keywords: COVID-19; alpha variant; children; household transmission.
Published by Elsevier Inc.
Figures
References
-
- Centers for Disease Control and Prevention COVID data tracker 2021. https://covid.cdc.gov/covid-data-tracker/#datatracker-home
-
- Dong Y., Mo X., Hu Y., Qi X., Jiang F., Jiang Z., et al. Epidemiology of COVID-19 among children in China. Pediatrics. 2020;145:e20200702. - PubMed
-
- Laws R.L., Chancey R.J., Rabold E.M., Chu V.T., Lewis N.M., Fajans M., et al. Symptoms and transmission of SARS-CoV-2 among children—Utah and Wisconsin, March-May 2020. Pediatrics. 2021;147 :e2020027268. - PubMed
