

Hypertension and Arrhythmias: A Clinical Overview of the Pathophysiology-Driven Management of Cardiac Arrhythmias in Hypertensive Patients
- PMID: 35448086
- PMCID: PMC9025699
- DOI: 10.3390/jcdd9040110
Hypertension and Arrhythmias: A Clinical Overview of the Pathophysiology-Driven Management of Cardiac Arrhythmias in Hypertensive Patients
Abstract
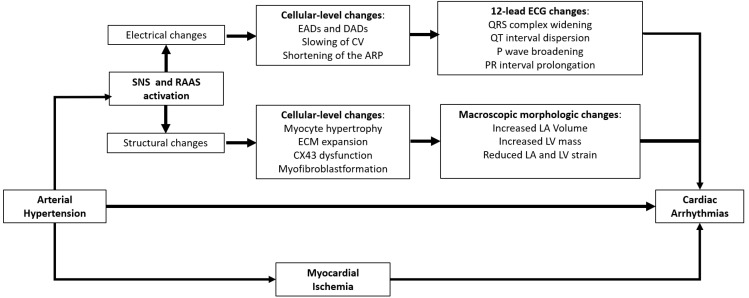
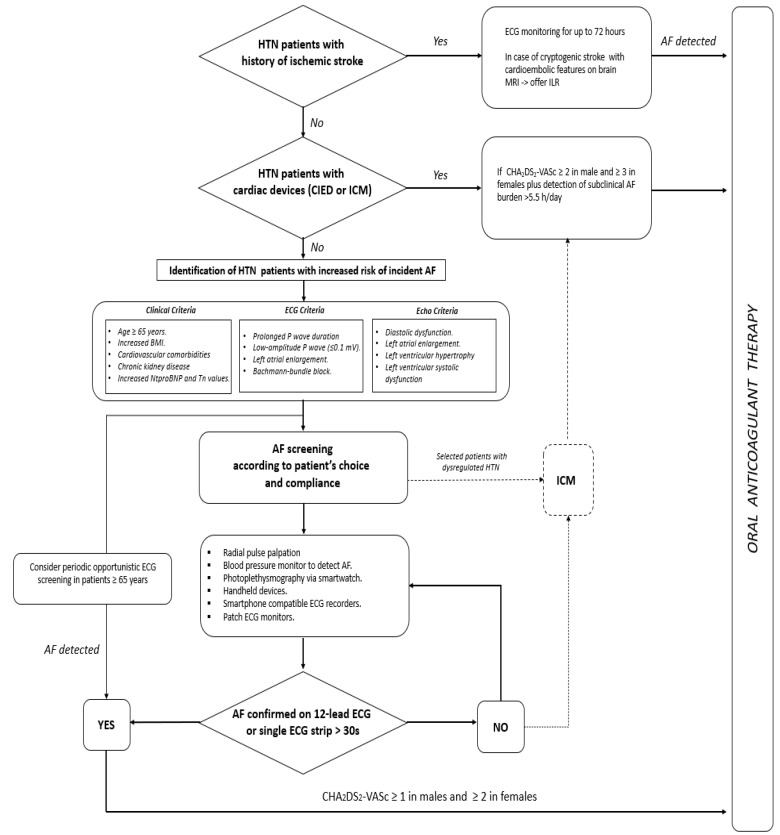
Because of demographic aging, the prevalence of arterial hypertension (HTN) and cardiac arrhythmias, namely atrial fibrillation (AF), is progressively increasing. Not only are these clinical entities strongly connected, but, acting with a synergistic effect, their association may cause a worse clinical outcome in patients already at risk of ischemic and/or haemorrhagic stroke and, consequently, disability and death. Despite the well-known association between HTN and AF, several pathogenetic mechanisms underlying the higher risk of AF in hypertensive patients are still incompletely known. Although several trials reported the overall clinical benefit of renin-angiotensin-aldosterone inhibitors in reducing incident AF in HTN, the role of this class of drugs is greatly reduced when AF diagnosis is already established, thus hinting at the urgent need for primary prevention measures to reduce AF occurrence in these patients. Through a thorough review of the available literature in the field, we investigated the basic mechanisms through which HTN is believed to promote AF, summarising the evidence supporting a pathophysiology-driven approach to prevent this arrhythmia in hypertensive patients, including those suffering from primary aldosteronism, a non-negligible and under-recognised cause of secondary HTN. Finally, in the hazy scenario of AF screening in hypertensive patients, we reviewed which patients should be screened, by which modality, and who should be offered oral anticoagulation for stroke prevention.
Keywords: anticoagulants; antihypertensive agents; artificial pacemakers; atrial fibrillation; hypertension; primary hyperaldosteronism.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
Hypertension and Atrial Fibrillation: Doubts and Certainties From Basic and Clinical Studies.Circ Res. 2018 Jan 19;122(2):352-368. doi: 10.1161/CIRCRESAHA.117.311402. Circ Res. 2018. PMID: 29348255 Review.
-
Atrial Fibrillation and Hypertension: Mechanistic, Epidemiologic, and Treatment Parallels.Methodist Debakey Cardiovasc J. 2015 Oct-Dec;11(4):228-34. doi: 10.14797/mdcj-11-4-228. Methodist Debakey Cardiovasc J. 2015. PMID: 27057292 Free PMC article. Review.
-
Arterial hypertension in patients with atrial fibrillation in Europe: A report from the EURObservational Research Programme pilot survey on atrial fibrillation.Int J Cardiol. 2018 Mar 1;254:136-141. doi: 10.1016/j.ijcard.2017.10.092. Epub 2018 Jan 28. Int J Cardiol. 2018. PMID: 29407080
-
Hypertension and atrial fibrillation: a bench to bedside perspective.Front Biosci (Schol Ed). 2018 Mar 1;10(2):276-284. doi: 10.2741/s515. Front Biosci (Schol Ed). 2018. PMID: 29293432 Review.
-
Relationship of Hypertension and Systolic Blood Pressure With the Risk of Stroke or Bleeding in Patients With Atrial Fibrillation: The Fushimi AF Registry.Am J Hypertens. 2017 Nov 1;30(11):1073-1082. doi: 10.1093/ajh/hpx094. Am J Hypertens. 2017. PMID: 28575205
Cited by
-
Controls of Central and Peripheral Blood Pressure and Hemorrhagic/Hypovolemic Shock.J Clin Med. 2023 Jan 31;12(3):1108. doi: 10.3390/jcm12031108. J Clin Med. 2023. PMID: 36769755 Free PMC article. Review.
-
New Perspectives and Strategies for the Management of Hypertension.J Cardiovasc Dev Dis. 2023 Aug 14;10(8):346. doi: 10.3390/jcdd10080346. J Cardiovasc Dev Dis. 2023. PMID: 37623359 Free PMC article.
-
Exploring the relationship between nocturnal hypertension and atrial fibrillation recurrence.Hypertens Res. 2024 Jul;47(7):1973-1975. doi: 10.1038/s41440-024-01694-8. Epub 2024 May 8. Hypertens Res. 2024. PMID: 38720030 No abstract available.
-
Association between complete blood-count-based inflammatory scores and hypertension in persons living with and without HIV in Zambia.PLoS One. 2024 Nov 11;19(11):e0313484. doi: 10.1371/journal.pone.0313484. eCollection 2024. PLoS One. 2024. PMID: 39527564 Free PMC article.
-
Incidence and prevalence of hypertension in 18-40-year-old patients referred for palpitations with normal cardiac monitor findings.J Clin Hypertens (Greenwich). 2024 Jun;26(6):696-702. doi: 10.1111/jch.14813. Epub 2024 Apr 19. J Clin Hypertens (Greenwich). 2024. PMID: 38641880 Free PMC article.
References
-
- Williams B., Mancia G., Spiering W., Agabiti Rosei E., Azizi M., Burnier M., Clement D.L., Coca A., de Simone G., Dominiczak A., et al. ESC/ESH Guidelines for the Management of Arterial Hypertension, The Task Force for the Management of Arterial Hypertension of the European Society of Cardiology and the European Society of Hypertension, The Task Force for the Management of Arterial Hypertension of the European Society of Cardiology and the European Society of Hypertension. J. Hypertens. 2018;36:1953–2041. doi: 10.1097/HJH.0000000000001940. - DOI - PubMed
-
- Chow C.K., Teo K.K., Rangarajan S., Islam S., Gupta R., Avezum A., Bahonar A., Chifamba J., Dagenais G., Diaz R., et al. PURE Study Investigators. Prevalence, awareness, treatment, and control of hypertension in rural and urban communities in high-, middle-, and low-income countries. JAMA. 2013;310:959–968. doi: 10.1001/jama.2013.184182. - DOI - PubMed
-
- Lip G.Y.H., Coca A., Kahan T., Boriani G., Manolis A.S., Olsen M.H., Oto A., Potpara T.S., Steffel J., Marín F., et al. Hypertension and cardiac arrhythmias, A consensus document from the European Heart Rhythm Association (EHRA) and ESC Council on Hypertension, endorsed by the Heart Rhythm Society (HRS), Asia-Pacific Heart Rhythm Society (APHRS) and Sociedad Latinoamericana de Estimulacion Cardiaca y Electrofisiologia (SOLEACE) Europace. 2017;19:891–911. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
