

The role of MRI in the diagnosis and management of tracheal diverticulum
- PMID: 35448959
- PMCID: PMC9027829
- DOI: 10.1186/s12880-022-00802-9
The role of MRI in the diagnosis and management of tracheal diverticulum
Abstract
Background: Multidetector CT is currently the best imaging method for detecting tracheal diverticulum (TD). Compared with CT, MRI is radiation-free and has higher resolution. However, the MRI characteristics of this disease have not been previously reported. The present retrospective study compared the MR and CT imaging features of TD, aiming to examine the role of MRI in TD diagnosis and management.
Methods: Imaging data were collected in 26 TD patients divided into two groups, including the uninfected and infected groups. The MR and CT imaging features (size/wall/channel) of uninfected patients were compared. The performances of MRI and CT in diagnosing and monitoring therapeutic efficacy in infected TD patients were comparatively assessed.
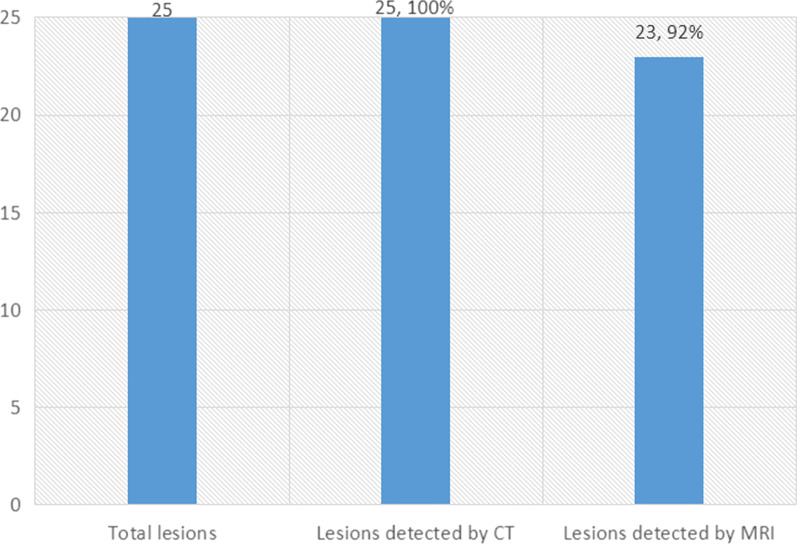
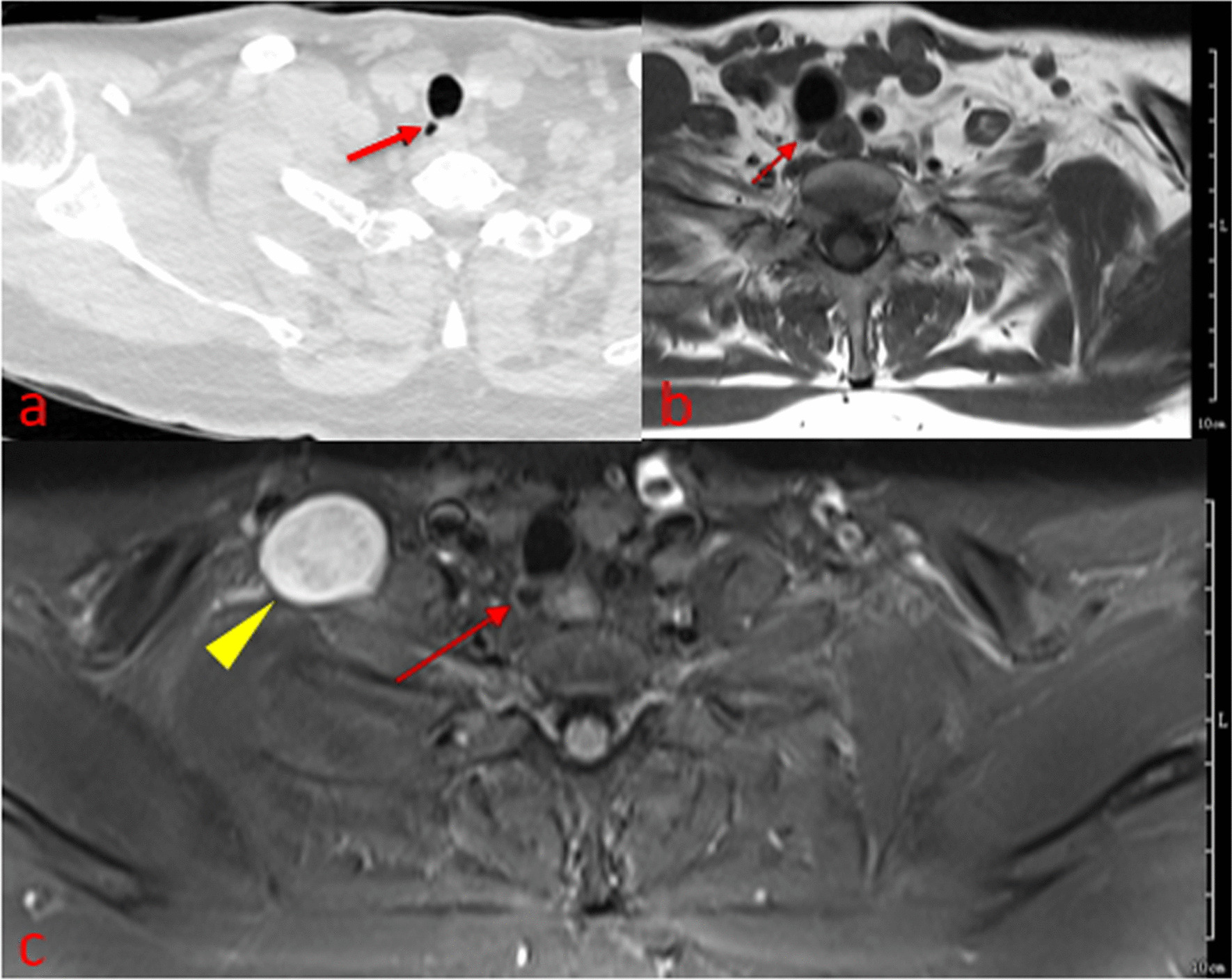
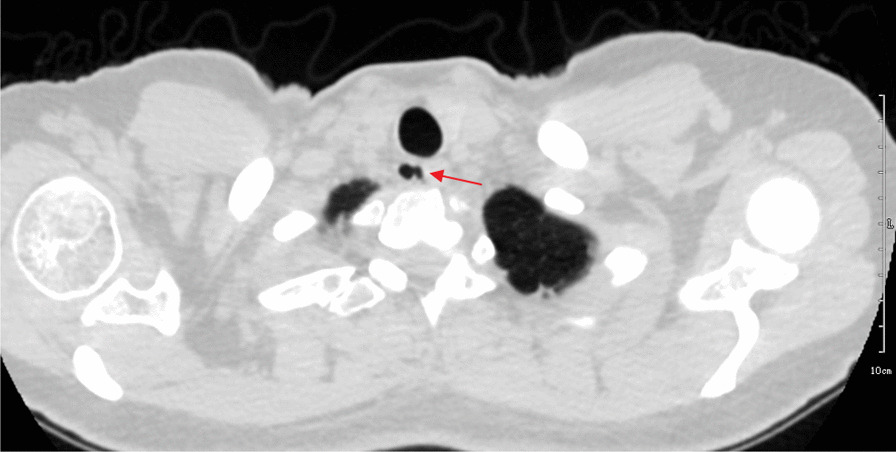
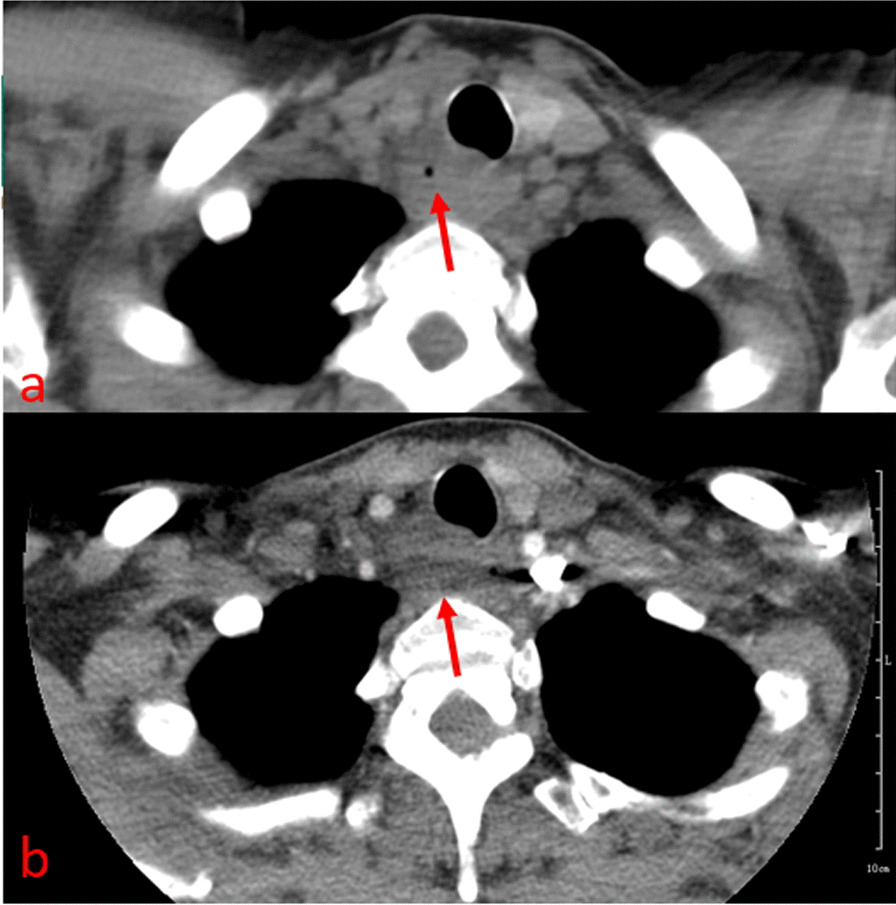
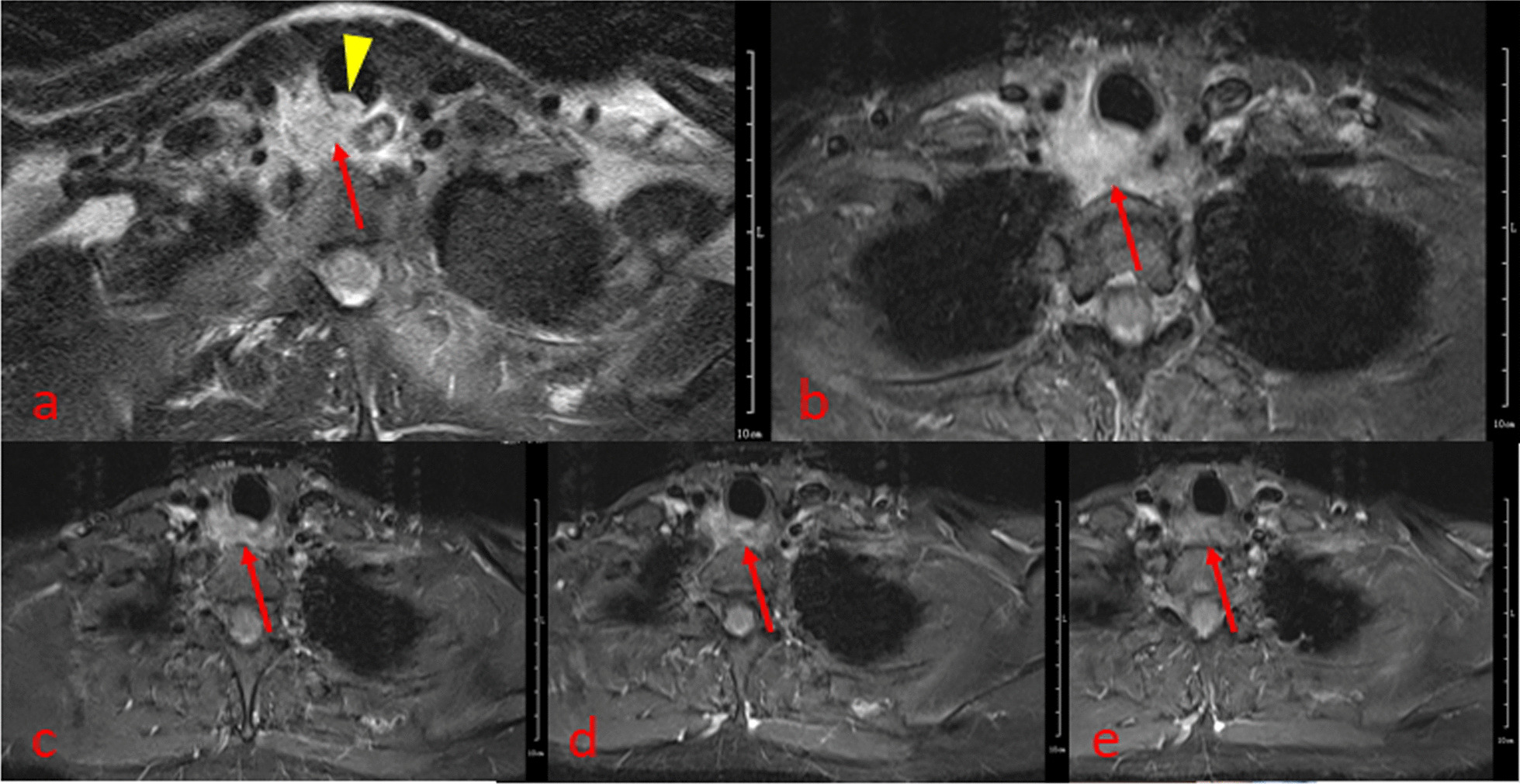
Results: The uninfected group comprised 25 cases with 25 lesions confirmed by CT, including 23 lesions (92%) detected by MRI, with an average diameter of 8.5 mm (range from 3 to 15 mm). Meanwhile, the average diameter was 7.8 mm as measured by CT (range from 2.8 mm to 14.7 mm). The lesion diameters of the two cases not detected by MRI were 2.3 mm and 2 mm. MRI detected walls of all the 23 lesions (23/23), while CT detected no wall (0/23). CT showed channels in 18 lesions (18/23) versus3 for MRI (3/23). The infected case presented with a paratracheal abscess; MRI clearly showed a relationship between the abscess and the trachea, while CT could not show the lesion source. MRI also sensitively showed the whole process of lesion absorption.
Conclusions: MRI can be used as a supplementary method for TD diagnosis, providing information about the wall that cannot be obtained by CT. MRI is superior to CT in diagnosing infected TD cases presenting with a paratracheal abscess, and in monitoring therapeutic efficacy in these patients.
Keywords: CT; MRI; Paratracheal air cyst; Tracheal diverticula.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
The Role of MRI in Diagnosing and Managing Tracheal Diverticulum.Acad Radiol. 2021 Aug 13:S1076-6332(21)00323-8. doi: 10.1016/j.acra.2021.07.015. Online ahead of print. Acad Radiol. 2021. PMID: 34400080
-
Tracheal diverticula: A retrospective analysis of patients referred for thoracic CT.Medicine (Baltimore). 2018 Sep;97(39):e12544. doi: 10.1097/MD.0000000000012544. Medicine (Baltimore). 2018. PMID: 30278548 Free PMC article.
-
Tracheal Diverticula.Semin Ultrasound CT MR. 2016 Jun;37(3):190-5. doi: 10.1053/j.sult.2016.04.002. Epub 2016 Apr 8. Semin Ultrasound CT MR. 2016. PMID: 27261344 Review.
-
A right paratracheal air cyst caused by tracheal diverticula.Intern Med. 2010;49(4):315-9. doi: 10.2169/internalmedicine.49.2731. Epub 2010 Feb 15. Intern Med. 2010. PMID: 20154437
-
Tracheal diverticulum: a case report and literature review.Am J Otolaryngol. 2014 Jul-Aug;35(4):542-5. doi: 10.1016/j.amjoto.2014.03.015. Epub 2014 Mar 26. Am J Otolaryngol. 2014. PMID: 24767473 Review.
Cited by
-
Tracheal Diverticula in People with Cystic Fibrosis on Elexacaftor/Tezacaftor/Ivacaftor: An Italian Multicenter Retrospective Study.J Clin Med. 2025 Mar 28;14(7):2320. doi: 10.3390/jcm14072320. J Clin Med. 2025. PMID: 40217771 Free PMC article.
-
Case report: tracheobronchial diverticulum, a potential risk for diving?Front Med (Lausanne). 2024 Jan 11;10:1340974. doi: 10.3389/fmed.2023.1340974. eCollection 2023. Front Med (Lausanne). 2024. PMID: 38274443 Free PMC article.
-
Valsalva Maneuver during Computed Tomography for the Diagnosis of Tracheal Diverticulum: A Case Report.Cureus. 2024 Oct 30;16(10):e72726. doi: 10.7759/cureus.72726. eCollection 2024 Oct. Cureus. 2024. PMID: 39618673 Free PMC article.
-
Tracheal Diverticulum Mimicking Pneumomediastinum: A Case Report Emphasizing the Importance of Differential Diagnosis in Chest Imaging Evaluation.Cureus. 2023 May 21;15(5):e39297. doi: 10.7759/cureus.39297. eCollection 2023 May. Cureus. 2023. PMID: 37346209 Free PMC article.
References
-
- Haghi Z, Towhidi M, Fattahi H, et al. Right paratracheal air cyst (tracheal diverticulum) Respir Care. 2009;54(10):1409–1411. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
