

Long delay in diagnosis of a case with MEN1 due to concomitant presence of AIMAH with insulinoma: a case report and literature review
- PMID: 35448982
- PMCID: PMC9022315
- DOI: 10.1186/s12902-022-01022-6
Long delay in diagnosis of a case with MEN1 due to concomitant presence of AIMAH with insulinoma: a case report and literature review
Abstract
Background: ACTH-independent macronodular hyperplasia (AIMAH) is an uncommon disorder characterized by massive enlargement of both adrenal glands and hypersecretion of cortisol. Concomitant AIMAH and multiple endocrine neoplasia type1 (MEN1) is rare to our knowledge.
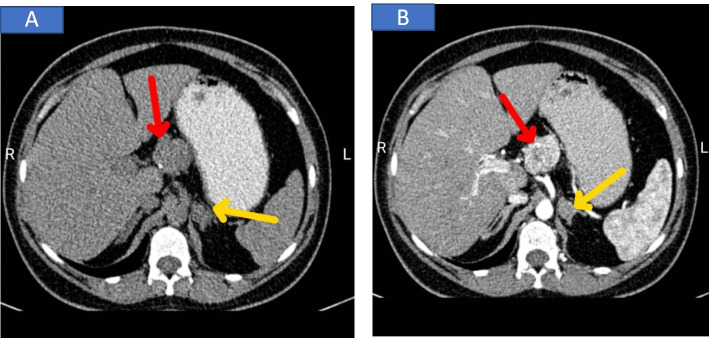
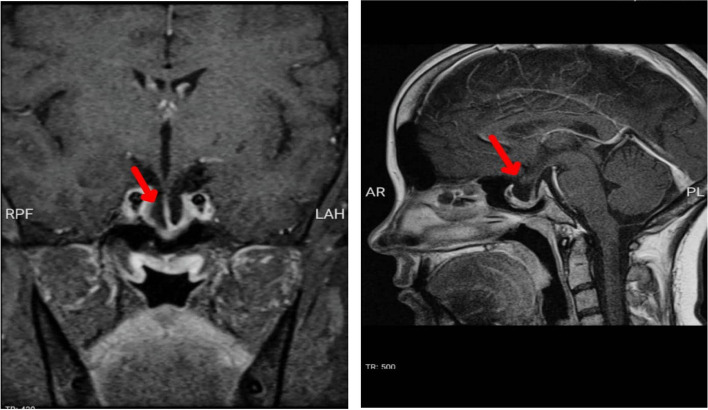
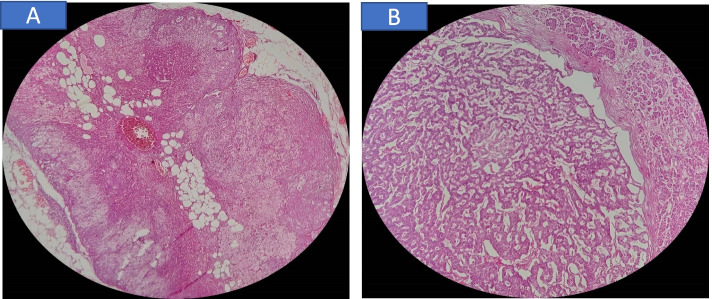
Case presentation: Herein, we describe a 32 year old woman with long history of prolactinoma and secondary ammonhrea presented with not-severe manifestation of hypoglycemia due to concomitant presence of insulinoma with AIMAH leading to 12 years delay of MEN1 diagnosis. Laboratory tests showed severe hypoglycemia associated with hyper insulinemia (non-fasting blood sugar = 43 mg/dl, insulin = 80.6 μIU /ml, C-peptide = 9.3 ng/ml) hyperparathyroidism (calcium = 10.3 mg/dl, phosphor = 3.1 mg/dl, PTH = 280 pg/ml) and chemical evidence of an ACTH-independent hypercortisolism (serum cortisol value of 3.5, after 1 mg dexamethasone suppression test serum ACTH value of 17 pg/ml, and high urinary cortisol level). Abdominal CT scan demonstrated two enhancing well-defined masses 27*20 mm and 37*30 mm in the tail and body of the pancreas, respectively, and a 36*15 mm mass in left adrenal gland (seven Hounsfield units). Dynamic pituitary MRI revealed a partial empty sella. The physical examination of the patient was unremarkable. Distal pancreatectomy and a left adrenalectomy were performed. After the surgery, we observed clinical and biochemical remission of hyper insulinemia and gradual decrease in urinary cortisol. The histological features of the removed left adrenal gland were consistent with AIMAH. Histological examination of the pancreatic lesions revealed well differentiated neuroendocrine tumors. Genetic abnormalities in the MEN1, heterozygote for pathogenic variant chr11; 645,773,330-64577333AGAC, c.249-252delGTCT, p. (11e85Serfs Ter33) in exon 2 were found. It was recommended the patient undergoes parathyroidectomy as soon as possible.
Conclusion: Given the history and presentation of our case, we recommend that the clinicians consider the possibility of autonomous cortisol production in MEN1 patients who do not show severe symptoms of hypoglycemia in the presence of insulinoma.
Keywords: AIMAH; Case report; Genetic mutation; Insulinoma; MEN-1.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Lacroix A, Bourdeau I. Bilateral adrenal Cushing’s syndrome: macronodular adrenal hyperplasia and primary pigmented nodular adrenocortical disease. Endocrinol Metab Clin. 2005;34(2):441–58. - PubMed
-
- Stratakis CA, Boikos SA. Genetics of adrenal tumors associated with Cushing’s syndrome: a new classification for bilateral adrenocortical hyperplasias. Nat Clin Pract Endocrinol Metab. 2007;3(11):748–57. - PubMed
-
- Ohashi A, Yamada Y, Sakaguchi K, Inoue T, Kubo M. FUSHIMI H: A natural history of adrenocorticotropin-independent bilateral adrenal macronodular hyperplasia (AIMAH) from preclinical to clinically overt Cushing’s syndrome. Endocr J. 2001;48(6):677–83. - PubMed
-
- Findlay JC, Sheeler LR, Engeland WC, Aron DC. Familial adrenocorticotropin-independent Cushing’s syndrome with bilateral macronodular adrenal hyperplasia. J Clin Endocrinol Metab. 1993;76(1):189–91. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
