

STRONG for Surgery & Strong for Life - against all odds: intensive prehabilitation including smoking, nutrition, alcohol and physical activity for risk reduction in cancer surgery - a protocol for an RCT with nested interview study (STRONG-Cancer)
- PMID: 35449008
- PMCID: PMC9027477
- DOI: 10.1186/s13063-022-06272-2
STRONG for Surgery & Strong for Life - against all odds: intensive prehabilitation including smoking, nutrition, alcohol and physical activity for risk reduction in cancer surgery - a protocol for an RCT with nested interview study (STRONG-Cancer)
Abstract
Background: There is a large unused potential for risk reduction in the preoperative period via effective lifestyle intervention targeting co-existing risky lifestyles: Smoking, malNutrition, obesity, risky Alcohol intake and insufficient Physical activity (SNAP). This trial compares the efficacy of the integrated STRONG programme with standard care on preoperative risk reduction and secondly on SNAP factor improvement and frailty, postoperative complications and quality of life. A nested interview study explores the patient preferences and the multi-perspective view of patients, relatives and health professionals.
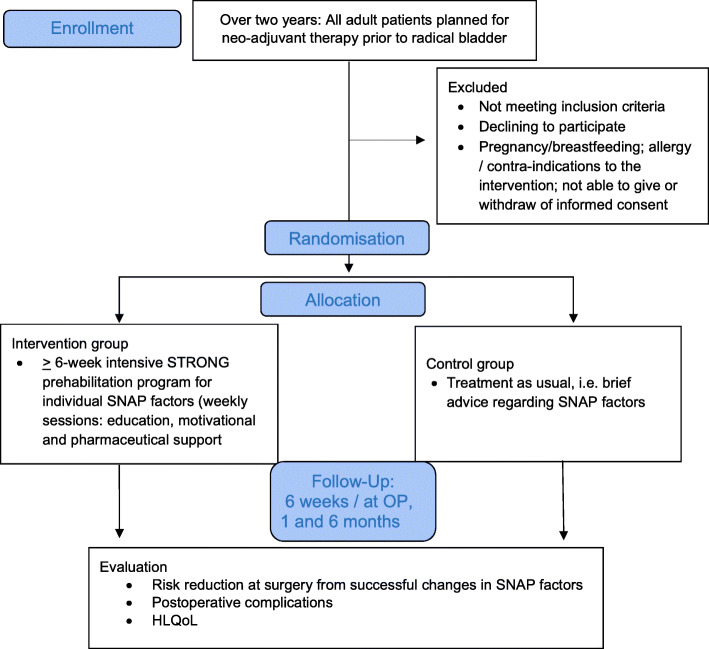
Methods: In total, 42 surgical patients with ≥1 SNAP factor are allocated to individually tailored STRONG programme or usual care during adjuvant chemotherapy prior to radical bladder cancer surgery. The STRONG programme has ≥6 weekly sessions with patient education, motivational and pharmaceutical support. It is based on intensive smoking and alcohol cessation interventions reporting perioperative quit rates > 50%. Surgical risk reduction is measured as ≥1 step for 1 or more risky lifestyles on the ASA-score, secondly as having no risky SNAP factors, and as any SNAP improvement. The outcomes are validated by measurements and biomarkers. Postoperative complications are categorised according to the Clavien-Dindo classification. Health-related quality of life is measured by EQ-5D. The patients are followed up after 6 weeks at surgery and 6 weeks and 6 months postoperatively. A representative sample of the participants, their relatives and the clinical staff are interviewed until data saturation. Transcription, triangulated analyses and data management are conducted using NVivo computer software.
Discussion: The surgical agenda is characterised by fixed dates for surgery focusing on clear risk reduction within a short time. This requires a clinical useful lifestyle intervention programme with a high effect and coverage as well as containing all SNAP factors and tailored to individual needs. The STRONG programme seems to meet these requirements. After development in multi-professional collaboration, STRONG is delivered by a specially trained nurse as part of the surgical patient journey. Overall, this study will bring important new knowledge about risk reduction in a frail patient group undergoing major cancer surgery.
Trial registration: Registration at www.clintrials.gov ( NCT04088968 ) The manuscript form from https://trialsjournal.biomedcentral.com/bmc/journal and the SPIRIT guidelines are followed.
Keywords: Alcohol drinking; Bladder cancer; Malnutrition; Obesity; Overweight; Perioperative risk reduction; Physical activity; Prehabilitation; Radical cystectomy; Smoking.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Effect of tailored, intensive prehabilitation for risky lifestyles before ventral hernia repair on postoperative outcomes, health, and costs - study protocol for a randomised controlled trial (STRONG-Hernia).PLoS One. 2025 May 28;20(5):e0324002. doi: 10.1371/journal.pone.0324002. eCollection 2025. PLoS One. 2025. PMID: 40435308 Free PMC article.
-
PRehabIlitatiOn with pReoperatIve exercise and educaTion for patients undergoing major abdominal cancer surgerY: protocol for a multicentre randomised controlled TRIAL (PRIORITY TRIAL).BMC Cancer. 2022 Apr 22;22(1):443. doi: 10.1186/s12885-022-09492-6. BMC Cancer. 2022. PMID: 35459100 Free PMC article.
-
EffectiveNess of a multimodal preHAbilitation program in patieNts with bladder canCEr undergoing radical cystectomy: protocol of the ENHANCE multicentre randomised controlled trial.BMJ Open. 2023 Mar 7;13(3):e071304. doi: 10.1136/bmjopen-2022-071304. BMJ Open. 2023. PMID: 36882246 Free PMC article.
-
The Impact of Exercise and Nutrition as Part of a Person-Centered Approach to Prehabilitation in Patients with Bladder Cancer.Semin Oncol Nurs. 2020 Oct;36(5):151072. doi: 10.1016/j.soncn.2020.151072. Epub 2020 Sep 30. Semin Oncol Nurs. 2020. PMID: 33010983 Review.
-
The Potential of Prehabilitation in Radical Cystectomy Pathways: Where Are We Now?Semin Oncol Nurs. 2021 Feb;37(1):151107. doi: 10.1016/j.soncn.2020.151107. Epub 2021 Jan 12. Semin Oncol Nurs. 2021. PMID: 33446382 Review.
Cited by
-
Study of the significance of the combination of the fibrinogen-albumin ratio and sarcopenia in predicting the prognosis of laryngeal cancer patients undergoing radical surgery.BMC Cancer. 2024 Oct 11;24(1):1265. doi: 10.1186/s12885-024-13039-2. BMC Cancer. 2024. PMID: 39394062 Free PMC article.
-
Perspectives on an Intensive Hospital-Based Smoking Cessation Intervention in Relation to Transurethral Resection of the Bladder Tumour (TURBT): Interviews with Patients, Relatives, and Clinicians.Int J Environ Res Public Health. 2025 Apr 3;22(4):555. doi: 10.3390/ijerph22040555. Int J Environ Res Public Health. 2025. PMID: 40283780 Free PMC article.
-
Optimizing Lifestyle Before and After Surgery: A Qualitative Stakeholder Analysis Among Healthcare Professionals.Am J Lifestyle Med. 2025 Jun 29:15598276251355917. doi: 10.1177/15598276251355917. Online ahead of print. Am J Lifestyle Med. 2025. PMID: 40606269 Free PMC article.
-
Identification of Alcohol Use Prior to Major Cancer Surgery: Timeline Follow Back Interview Compared to Four Other Markers.Cancers (Basel). 2024 Jun 18;16(12):2261. doi: 10.3390/cancers16122261. Cancers (Basel). 2024. PMID: 38927966 Free PMC article.
-
Perioperative Intensive Smoking Cessation Intervention Among Smokers Who Underwent Transurethral Resection of Bladder Tumor (TURBT) in Two Different Settings: A Randomized Controlled Trial.Cancers (Basel). 2025 Feb 19;17(4):713. doi: 10.3390/cancers17040713. Cancers (Basel). 2025. PMID: 40002306 Free PMC article.
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
