

A Fatal Case of Takotsubo Cardiomyopathy Secondary to Refractory Hypoglycemia in Severe Starvation: An Autopsy Case Report
- PMID: 35449611
- PMCID: PMC9012600
- DOI: 10.7759/cureus.23287
A Fatal Case of Takotsubo Cardiomyopathy Secondary to Refractory Hypoglycemia in Severe Starvation: An Autopsy Case Report
Abstract
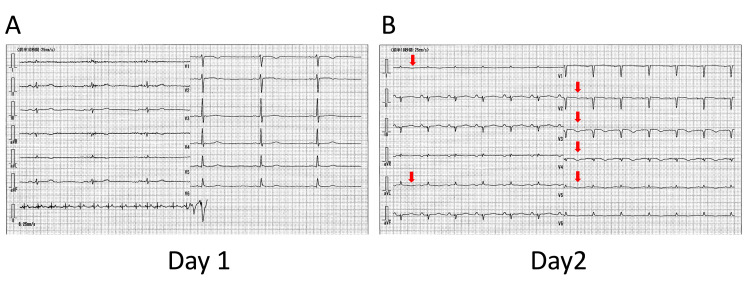
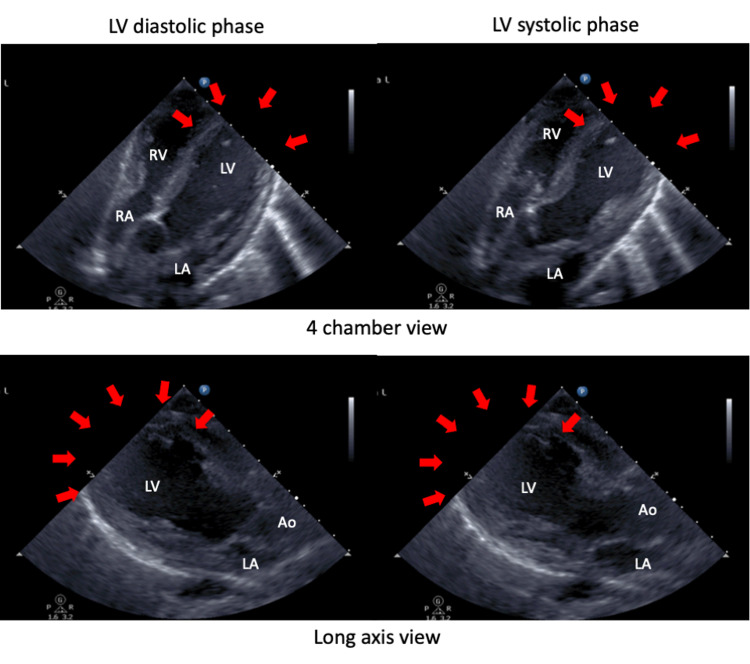
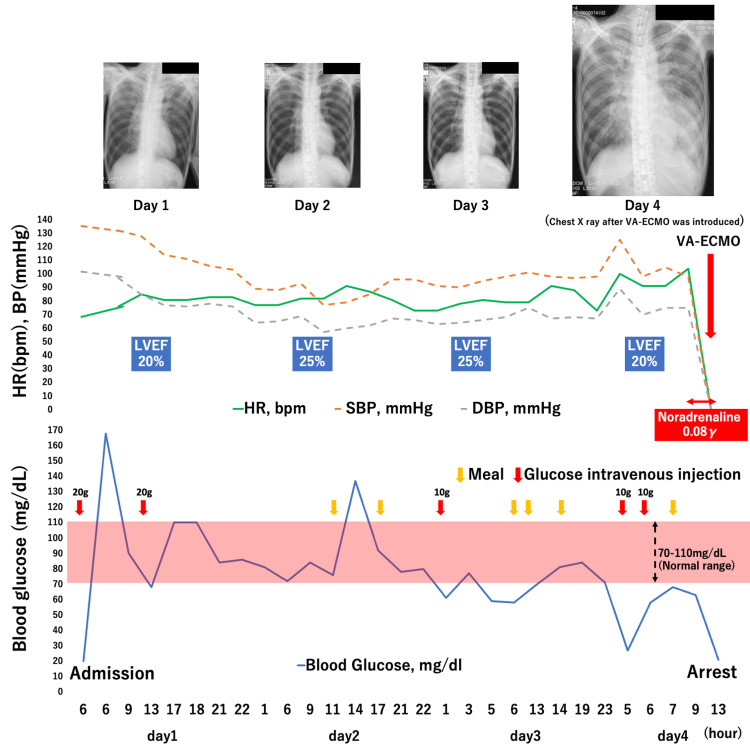
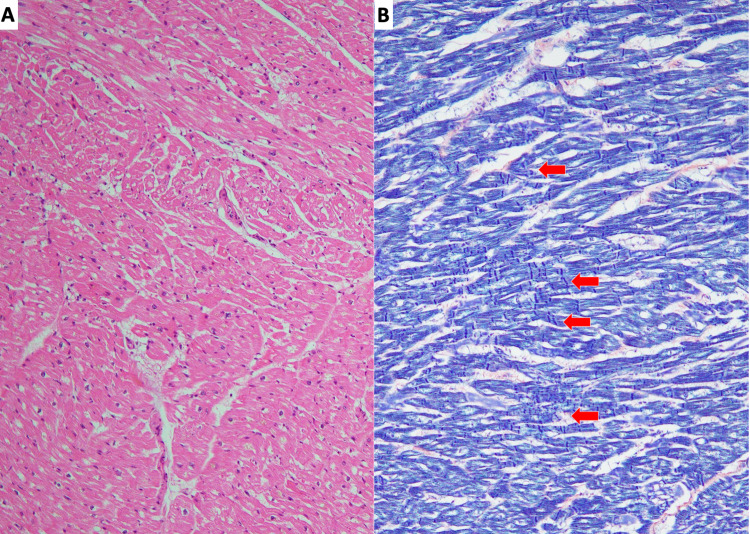
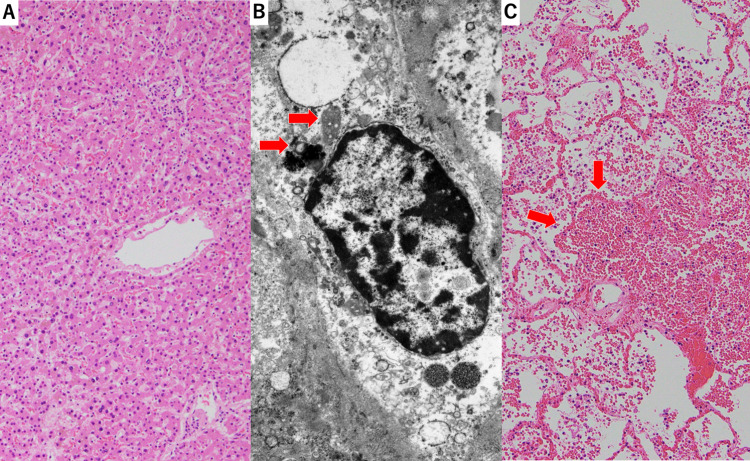
A 56-year-old, severely malnourished man presented with loss of consciousness due to hypoglycemia. Echocardiography revealed left ventricular apical ballooning, indicating takotsubo cardiomyopathy. Although his caloric intake was gradually increased to avoid refeeding syndrome, hypoglycemia was refractory, and repetitive glucose administration was required. On day 4 of admission, he developed severe refractory hypoglycemia with a progressive decrease in blood pressure. Consequently, pulseless ventricular tachycardia followed by pulseless electrical activity developed. Although venoarterial extracorporeal membrane oxygenation was introduced, the patient did not respond to the treatment and died. Autopsy revealed myocardial degeneration and contraction-band necrosis, indicative of takotsubo cardiomyopathy. No coronary stenosis was observed. The liver showed moderate hepatocyte atrophy and autophagosomes, consistent with starvation and not with refeeding syndrome. We speculated that refractory hypoglycemia induced extreme catecholamine secretion, which led to severe complications of takotsubo cardiomyopathy, such as fatal arrhythmia and extremely low cardiac output. Early recognition of these critically ill patients and timely therapeutic interventions, including strict glycemic control and adequate caloric intake, may improve patient outcomes.
Keywords: refeeding syndrome; refractory hypoglycemia; starvation; takotsubo cardiomyopathy; venoarterial extracorporeal membrane oxygenation (va-ecmo).
Copyright © 2022, Kirigaya et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Clinical features and outcomes of takotsubo (stress) cardiomyopathy. Templin C, Ghadri JR, Diekmann J, et al. N Engl J Med. 2015;373:929–938. - PubMed
-
- ASPEN consensus recommendations for refeeding syndrome. da Silva JS, Seres DS, Sabino K, et al. Nutr Clin Pract. 2020;35:178–195. - PubMed
-
- Hyperglycemia and subsequent torsades de pointes with marked QT prolongation during refeeding. Nakashima T, Kubota T, Takasugi N, et al. Nutrition. 2017;33:145–148. - PubMed
Publication types
LinkOut - more resources
Full Text Sources