

Effects of Sacubitril-Valsartan on Clinical, Echocardiographic, and Polygraphic Parameters in Patients Affected by Heart Failure With Reduced Ejection Fraction and Sleep Apnea
- PMID: 35449875
- PMCID: PMC9016131
- DOI: 10.3389/fcvm.2022.861663
Effects of Sacubitril-Valsartan on Clinical, Echocardiographic, and Polygraphic Parameters in Patients Affected by Heart Failure With Reduced Ejection Fraction and Sleep Apnea
Abstract
Background: Heart failure with reduced ejection fraction (HFrEF) is a clinical condition frequently diagnosed in clinical practice. In patients affected by HFrEF, sleep apnea (SA) can be detected among the most frequent comorbidities. Sacubitril-valsartan (sac/val) association has been proven to be effective in reducing disease progression and all-cause mortality in HFrEF patients. Sac/val treatment can potentially attenuate SA development via several pathophysiologic mechanisms, including improvement of global hemodynamics, reduction of extracellular fluid overload, and decrease of sympathetic neural activity.
Methods: We recruited 132 patients affected by HFrEF and SA, already under treatment with continuous positive airway pressure (CPAP), which was discontinued 24 h before the scheduled study timepoints. Physical examination, echocardiography, nocturnal cardio-respiratory monitoring, and laboratory tests were performed in each patient at baseline and after a 6-month treatment with sac/val.
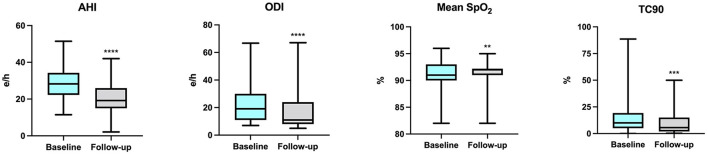
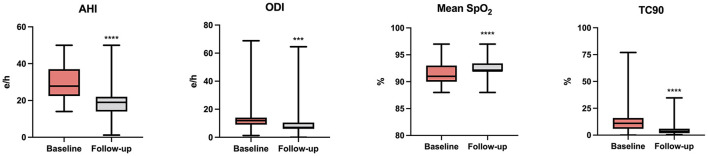
Results: After 6 months, sac/val induced statistically significant changes in clinical, hemodynamic, biohumoral (NT-proBNP, serum electrolytes, creatinine, and uric acid), and echocardiographic parameters. In particular, cardiac index (CI), both atrial and ventricular volumes and global longitudinal strain (GLS) improved. Moreover, polysomnography, carried out during a temporary CPAP interruption, revealed a significant reduction in global apnea-hypopnea index (AHI) value (p < 0.0001), central AHI (p < 0.0001), obstructive AHI (p < 0.0001), oxygen desaturation index (ODI) (p < 0.0001), and percentage time of saturation below 90% (TC90) (p < 0.0001). The changes of CI, estimated glomerular filtration rate (eGFR), NT-proBNP, and tricuspid annular plane excursion (TAPSE) contributed to 23.6, 7.6, 7.3, and 4.8% of AHI variability, respectively, and the whole model accounted for a 43.3% of AHI variation.
Conclusions: Our results suggest that treatment with sac/val is able to significantly improve the cardiorespiratory performance of patients with HFrEF and SA, integrating the positive impact of CPAP. Thus, both CPAP and sac/val therapy may synergistically contribute to lower the risks of both cardiac and pulmonary complications in HFrEF patients with SA.
Keywords: apnea-hypopnea index; echocardiography; heart failure; sacubitril-valsartan; sleep apnea.
Copyright © 2022 Pelaia, Armentaro, Volpentesta, Mancuso, Miceli, Caroleo, Perticone, Maio, Arturi, Imbalzano, Andreozzi, Perticone, Sesti and Sciacqua.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous