

Normalisation of airflow limitation in asthma: Post-hoc analyses of TRIMARAN and TRIGGER
- PMID: 35450196
- PMCID: PMC9014197
- DOI: 10.1002/clt2.12145
Normalisation of airflow limitation in asthma: Post-hoc analyses of TRIMARAN and TRIGGER
Abstract
Background: In asthma, persistent airflow limitation (PAL) is associated with poorer control, lung function decline and exacerbations. Using post-hoc analyses we evaluated: the relationship between post-salbutamol PAL at screening, airflow limitation (AL) during 52 weeks treatment with extrafine beclometasone dipropionate/formoterol fumarate/glycopyrronium (BDP/FF/G) versus BDP/FF and the risk of moderate/severe asthma exacerbations.
Methods: TRIMARAN and TRIGGER were double-blind studies comparing BDP/FF/G with BDP/FF (TRIMARAN medium-dose ICS; TRIGGER high-dose) in adults with uncontrolled asthma. Patients were subgrouped according to post-salbutamol PAL status at screening, and AL over the 52-week treatment period.
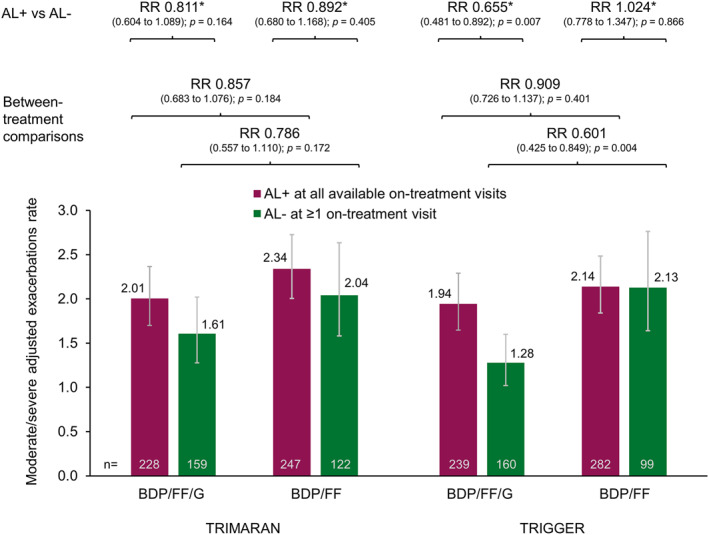
Results: Most patients with post-salbutamol PAL at screening had AL at all on-treatment visits (TRIMARAN 62.8%; TRIGGER 66.8%). A significantly higher proportion of patients had normalised airflow on ≥1 follow-up visit when receiving BDP/FF/G than BDP/FF (TRIMARAN 44.1 vs. 33.1% [p = 0.003]; TRIGGER 40.1 vs. 26.0% [p < 0.001]). In patients with post-salbutamol PAL at screening and normalised AL at ≥1 follow-up visit, exacerbation rates were 15% (p = 0.105) and 19% (p = 0.039) lower in TRIMARAN and TRIGGER versus those with AL on all visits. There was a trend to lower exacerbation rates in patients receiving BDP/FF/G than BDP/FF, particularly in patients in whom AL was normalised.
Conclusion: In these analyses, AL in asthma was associated with an increased exacerbation incidence. Inhaled triple therapy with extrafine BDP/FF/G was more likely to normalise airflow, and was associated with a trend to a lower exacerbation rate than BDP/FF, particularly in the subgroup of patients in whom treatment was associated with airflow normalisation.ClinicalTrials.gov: TRIMARAN, NCT02676076; TRIGGER, NCT02676089.
Keywords: exacerbations; inhaled corticosteroid; inhaled triple therapy; long‐acting beta2‐agonist; long‐acting muscarinic antagonist.
© 2022 The Authors. Clinical and Translational Allergy published by John Wiley & Sons Ltd on behalf of European Academy of Allergy and Clinical Immunology.
Conflict of interest statement
Alberto Papi reports grants, personal fees, non‐financial support and payment for advisory board membership, consultancy, payment for lectures, grants for research, and travel expenses reimbursement from Chiesi, AstraZeneca, GlaxoSmithKline, Boehringer Ingelheim, Mundipharma and TEVA, and personal fees and non‐financial support from Menarini, Novartis, Zambon and Sanofi, all outside the submitted work. Dave Singh reports personal fees from Chiesi during the conduct of the studies. Outside the submitted work, he reports personal fees from AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, Genentech, GlaxoSmithKline, Glenmark, Menarini, Mundipharma, Novartis, Peptinnovate, Pfizer, Pulmatrix, Theravance, and Verona. J. Christian Virchow reports personal fees from Chiesi during the conduct of the studies. In the past J. Christian Virchow has lectured and received honoraria from AstraZeneca, Avontec, Bayer, Bencard, Bionorica, Boehringer‐Ingelheim, Chiesi, Essex/Schering‐Plough, GSK, Janssen‐Cilag, Leti, MEDA, Merck, MSD, Mundipharma, Novartis, Nycomed/Altana, Pfizer, Revotar, Sanofi/Regeneron, Sandoz‐Hexal, Stallergens, TEVA, UCB/Schwarz‐Pharma, Zydus/Cadila and possibly others, and participated in advisory boards and received honoraria from Avontec, Boehringer‐Ingelheim, Chiesi, Essex/Schering‐Plough, GSK, Janssen‐Cilag, MEDA, MSD, Mundipharma, Novartis, Paul‐Ehrlich Institut, Regeneron, Revotar, Roche, Sanofi‐Aventis, Sanofi/Regeneron, Sandoz‐Hexal, TEVA, UCB/Schwarz‐Pharma and possibly others, and received funding for research from Deutsche Forschungsgesellschaft, Land Mecklenburg‐Vorpommern, GSK, and MSD, and has advised the Bemeinsame Bundesausschuss (GBA). G. Walter Canonica reports personal fees from A. Menarini, Alk‐Abello, Allergy Therapeutics, AstraZeneca‐Medimmune, Boehringer Ingelheim, Chiesi Farmaceutici, Genentech, Guidotti‐Malesci, Glaxo Smith Kline, Hal Allergy, Merck Sharp & Dome, Mundipharma, Novartis, Orion, Sanofi‐Aventis, Sanofi Genzyme/Regeneron, Stallergenes‐Greer, Uriach Pharma, Teva, Valeas, ViforPharma, all outside the submitted work. Andrea Vele is an employee of Chiesi, the sponsor of the studies. George Georges is an employee of Chiesi USA, Inc.
Figures



References
-
- Global Initiative For Asthma . Global Strategy for Asthma Management and Prevention; 2021. Accessed December 21, 2021. https://ginasthma.org/reports/
-
- Konstantellou E, Papaioannou AI, Loukides S, et al. Persistent airflow obstruction in patients with asthma: characteristics of a distinct clinical phenotype. Respir Med. 2015;109:1404‐1409. - PubMed
-
- Smith BM, Zhao N, Olivenstein R, Lemiere C, Hamid Q, Martin JG. Asthma and fixed airflow obstruction: long‐term trajectories suggest distinct endotypes. Clin Exp Allergy. 2021;51:39‐48. - PubMed
-
- Tonga KO, Chapman DG, Farah CS, et al. Reduced lung elastic recoil and fixed airflow obstruction in asthma. Respirology. 2020;25:613‐619. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
