

Pericoronary Adipose Tissue Attenuation, Low-Attenuation Plaque Burden, and 5-Year Risk of Myocardial Infarction
- PMID: 35450813
- PMCID: PMC9187595
- DOI: 10.1016/j.jcmg.2022.02.004
Pericoronary Adipose Tissue Attenuation, Low-Attenuation Plaque Burden, and 5-Year Risk of Myocardial Infarction
Abstract
Background: Pericoronary adipose tissue (PCAT) attenuation and low-attenuation noncalcified plaque (LAP) burden can both predict outcomes.
Objectives: This study sought to assess the relative and additive values of PCAT attenuation and LAP to predict future risk of myocardial infarction.
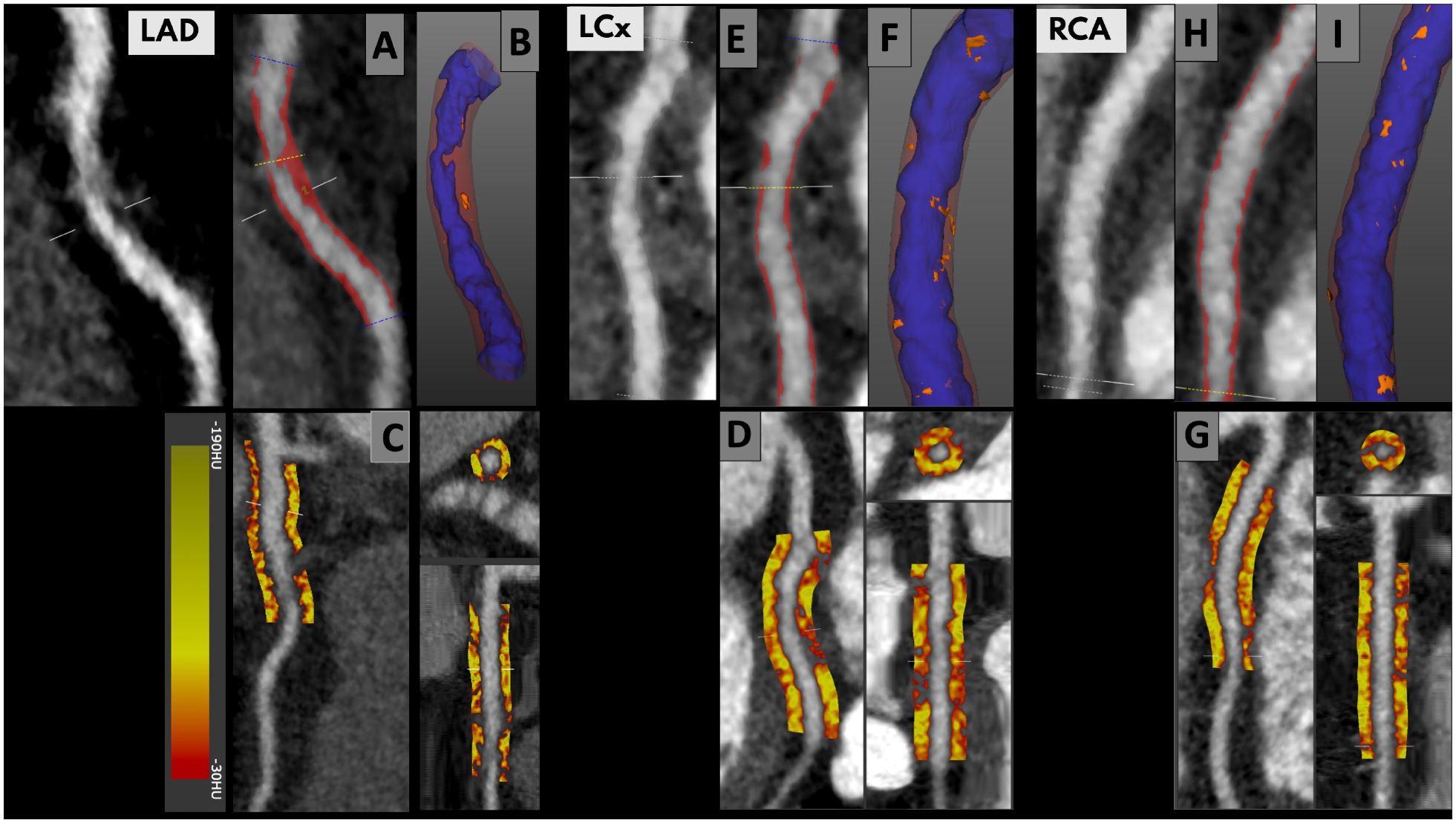
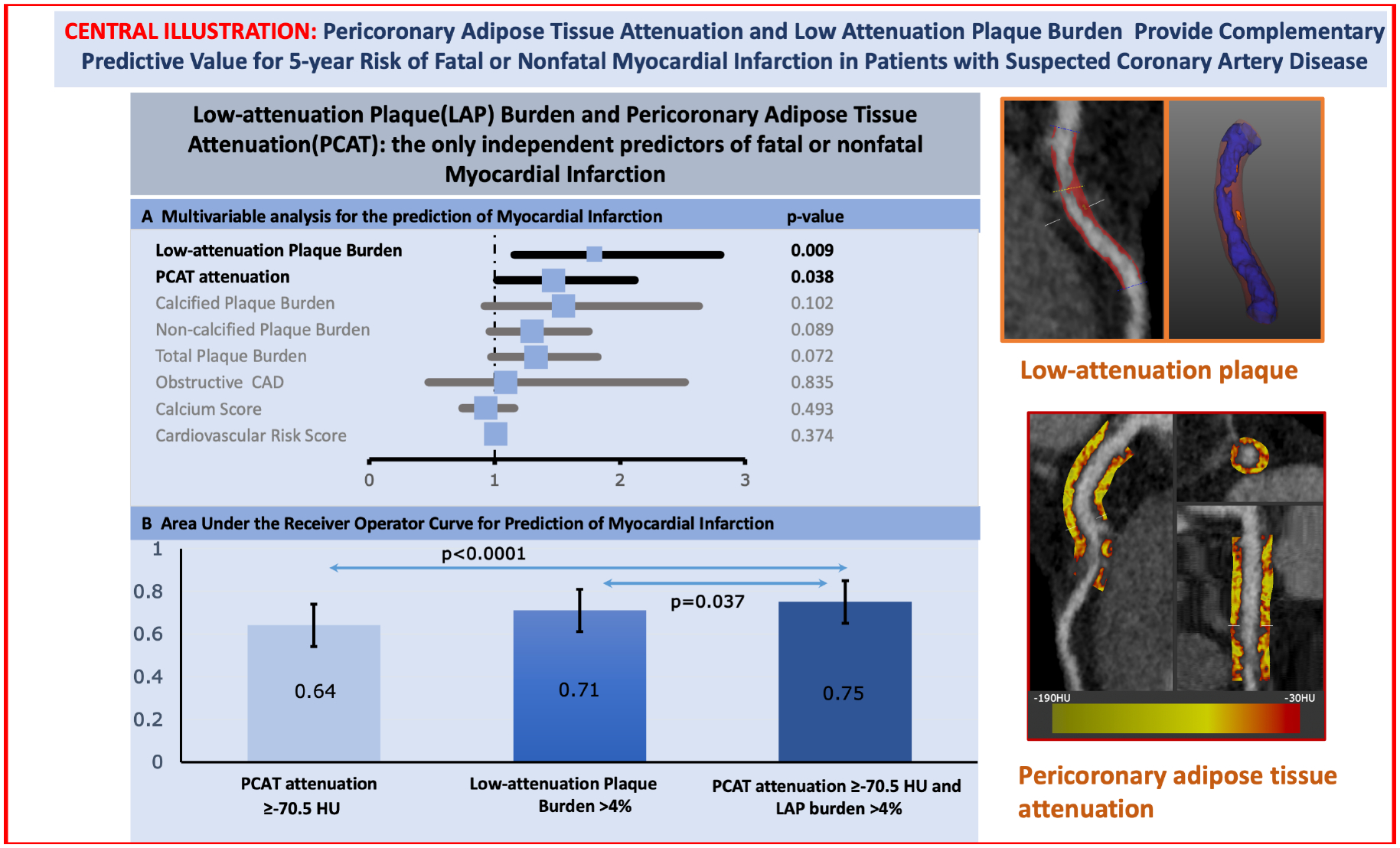
Methods: In a post hoc analysis of the multicenter SCOT-HEART (Scottish Computed Tomography of the Heart) trial, the authors investigated the relationships between the future risk of fatal or nonfatal myocardial infarction and PCAT attenuation measured from coronary computed tomography angiography (CTA) using multivariable Cox regression models including plaque burden, obstructive coronary disease, and cardiac risk score (incorporating age, sex, diabetes, smoking, hypertension, hyperlipidemia, and family history).
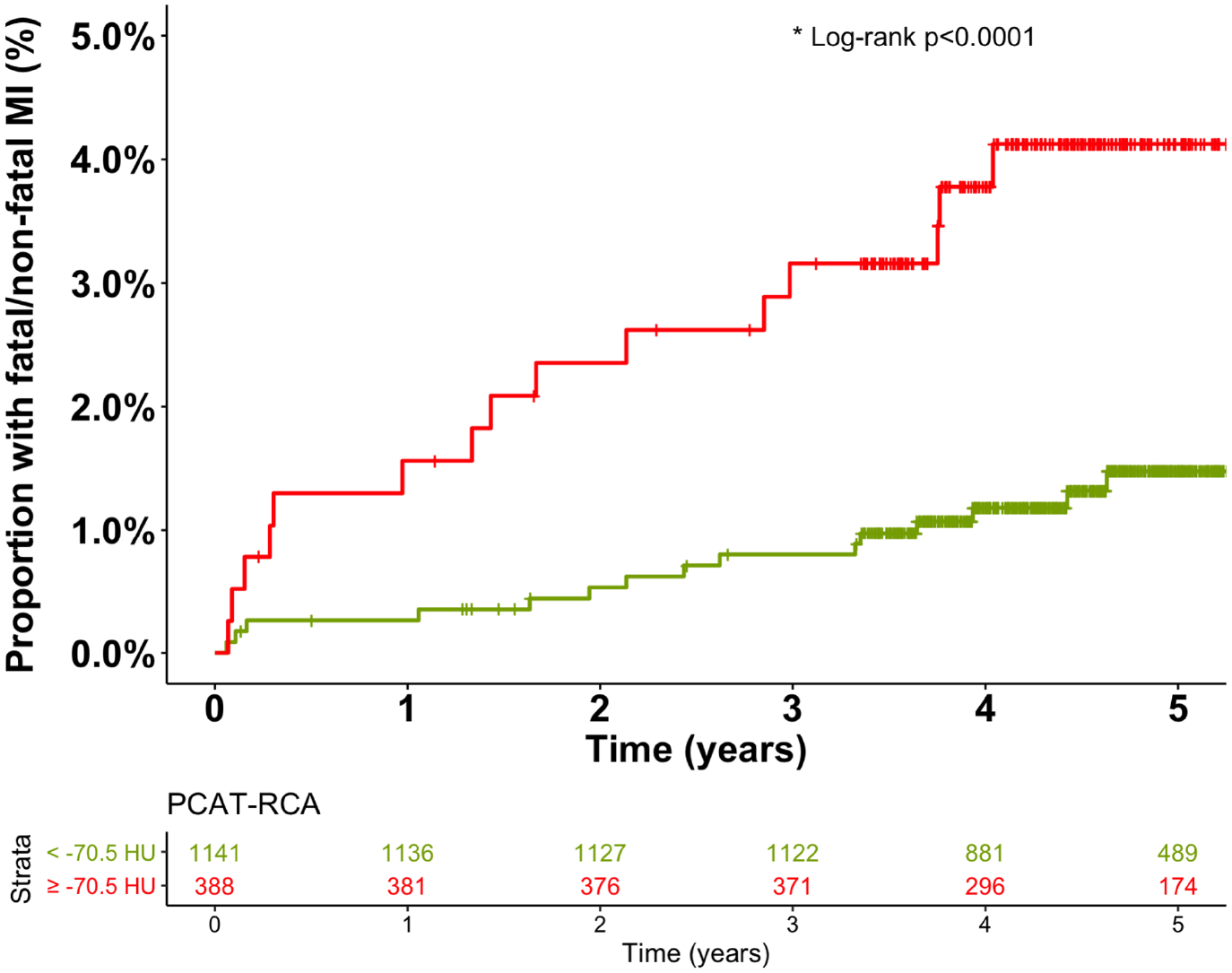
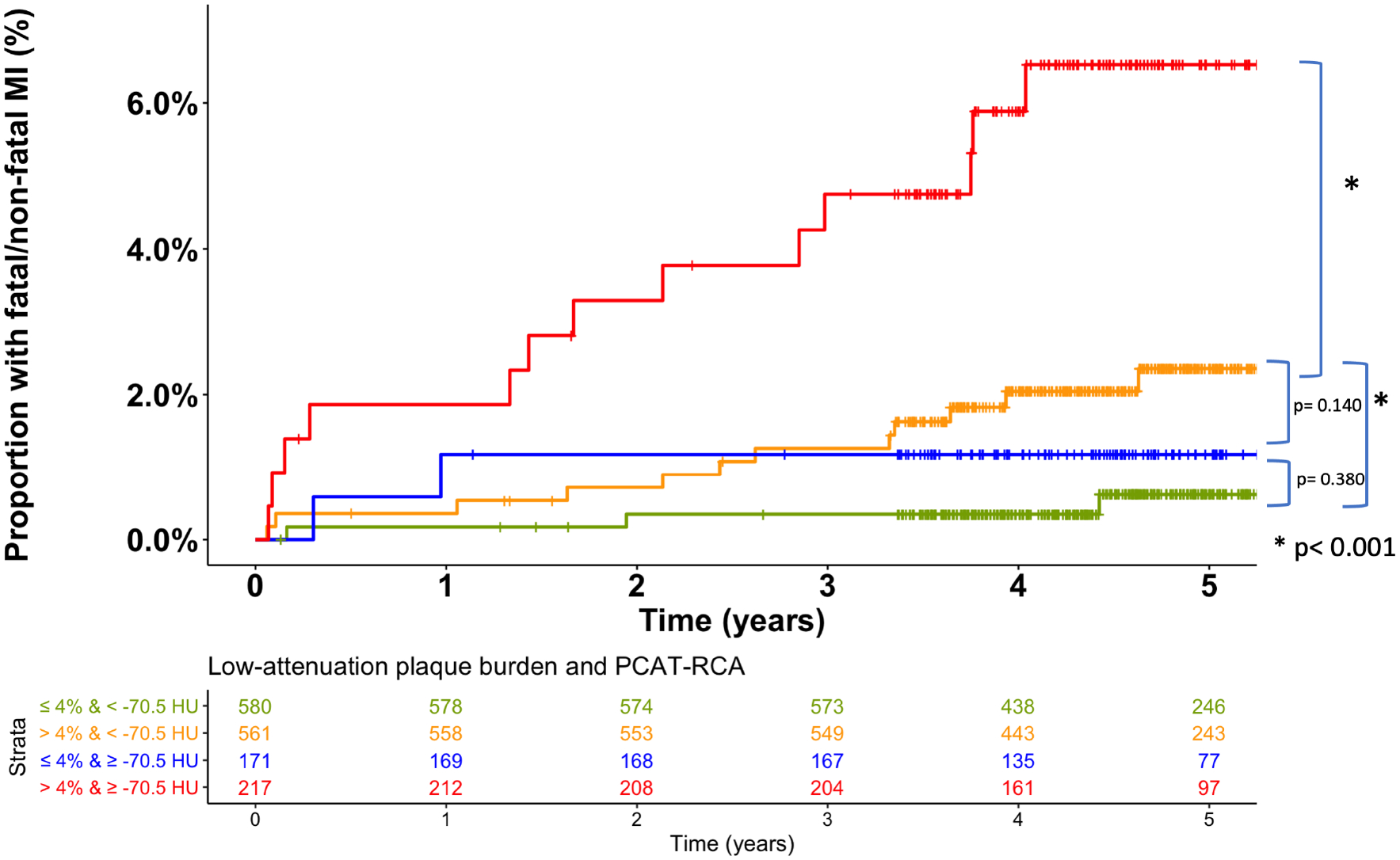
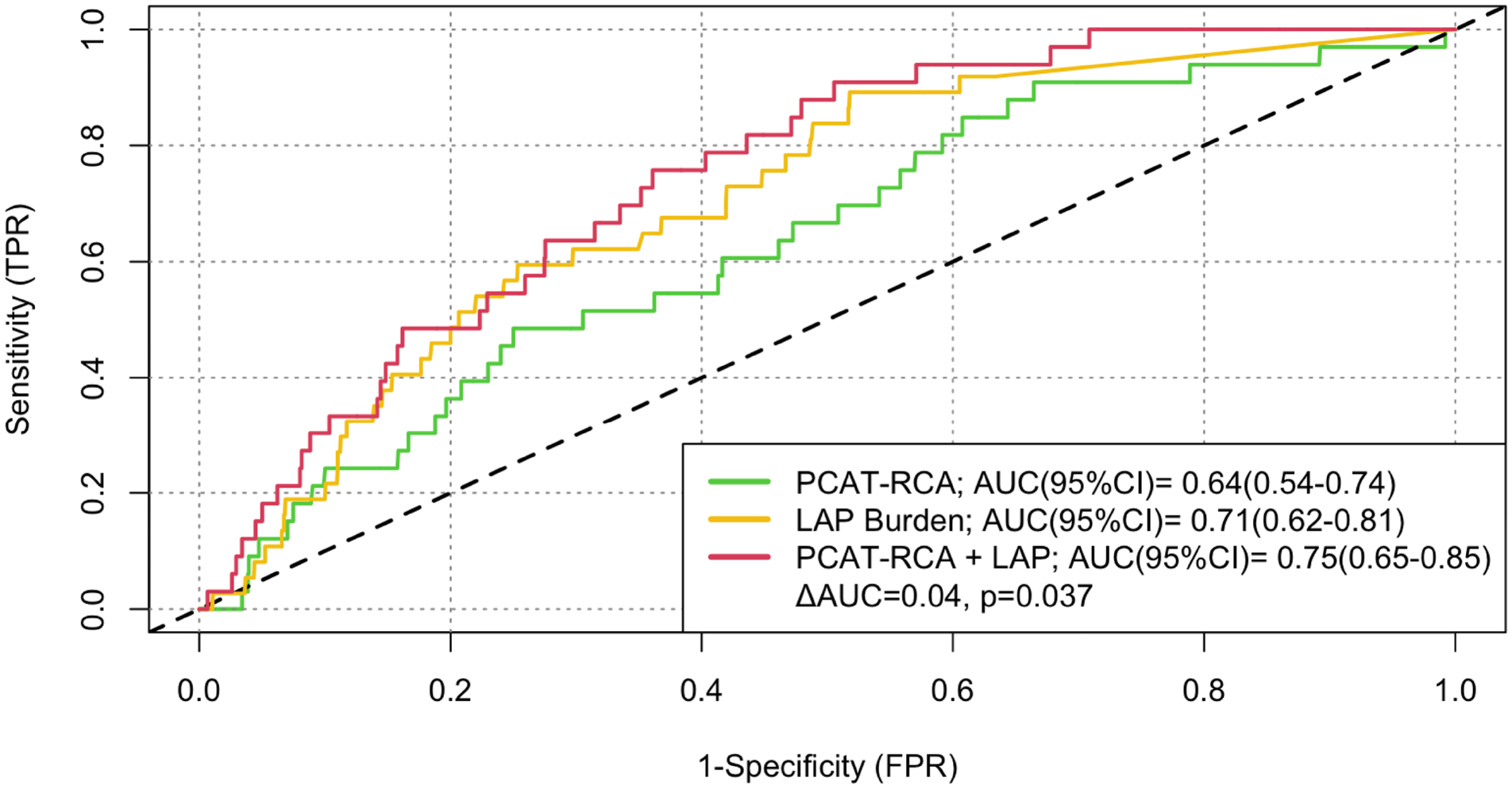
Results: In 1,697 evaluable participants (age: 58 ± 10 years), there were 37 myocardial infarctions after a median follow-up of 4.7 years. Mean PCAT was -76 ± 8 HU and median LAP burden was 4.20% (IQR: 0%-6.86%). PCAT attenuation of the right coronary artery (RCA) was predictive of myocardial infarction (HR: 1.55; P = 0.017, per 1 SD increment) with an optimum threshold of -70.5 HU (HR: 2.45; P = 0.01). In multivariable analysis, adding PCAT-RCA of ≥-70.5 HU to an LAP burden of >4% (the optimum threshold for future myocardial infarction; HR: 4.87; P < 0.0001) led to improved prediction of future myocardial infarction (HR: 11.7; P < 0.0001). LAP burden showed higher area under the curve compared to PCAT attenuation for the prediction of myocardial infarction (AUC = 0.71 [95% CI: 0.62-0.80] vs AUC = 0.64 [95% CI: 0.54-0.74]; P < 0.001), with increased area under the curve when the 2 metrics are combined (AUC = 0.75 [95% CI: 0.65-0.85]; P = 0.037).
Conclusion: Coronary CTA-defined LAP burden and PCAT attenuation have marked and complementary predictive value for the risk of fatal or nonfatal myocardial infarction.
Keywords: computed tomography angiography; coronary artery disease; low-attenuation noncalcified plaque burden; noncalcified plaque burden; pericoronary adipose tissue; risk stratification.
Copyright © 2022 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This trial was funded by The Chief Scientist Office of the Scottish Government Health and Social Care Directorates (CZH/4/588), with supplementary awards from Edinburgh and Lothian’s Health Foundation Trust and the Heart Diseases Research Fund. Dr Williams, (FS/ICRF/20/26002, FS/11/014, CH/09/002), Dr Newby (CH/09/002, RG/16/10/32375, RE/18/5/34216), and Dr Dweck (FS/14/78/31020) are supported by the British Heart Foundation. Dr Williams was supported by The Chief Scientist Office of the Scottish Government Health (PCL/17/04). Dr Newby is the recipient of a Wellcome Trust Senior Investigator Award (WT103782AIA). Dr van Beek is supported by the Scottish Imaging Network: A Platform of Scientific Excellence (SINAPSE). Dr Mills is supported by the British Heart Foundation through the award of the Butler Senior Clinical Research Fellowship and a Programme Grant (FS/16/14/32023, RG/20/10/34966). Dr Adamson is supported by a National Heart Foundation of New Zealand Senior Fellowship (1844). Dr Dweck is supported by the Sir Jules Thorn Biomedical Research Award 2015 (15/JTA). The Royal Bank of Scotland supported the provision of the 320-multidetector computed tomography for National Health Service Lothian and the University of Edinburgh. The Edinburgh Imaging Facility, The Queen's Medical Research Institute (Edinburgh) is supported by the National Health Service Research Scotland through the National Health Service Lothian Health Board. The Clinical Research Facility Glasgow and Clinical Research Facility Tayside are supported by National Health Service Research Scotland. This work is supported in part by the National Institutes of Health/National Heart, Lung, and Blood Institute grants 1R01HL148787-01A1 and 1R01HL151266. Drs Lin and Grodecki, Priscilla McElhinney, Sebastien Cadet, and Dr Dey are supported by National Institutes of Health/National Heart, Lung, and Blood Institute grant 1R01HL148787-01A1. This work is also supported in part by the Miriam and Sheldon G. Adelson Medical Research Foundation. Sebastien Cadet, and Drs Berman, Slomka, and Dey received software royalties from Cedars-Sinai Medical Center. Drs Slomka, Berman, and Dey hold a patent (US8885905B2 in the United States and World Intellectual Property Organization patent WO2011069120A1, “Method and System for Plaque Characterization”). All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Improving the Prediction of Major Clinical Cardiovascular Events With Cardiac Computed Tomographic Angiography.JACC Cardiovasc Imaging. 2022 Jun;15(6):1089-1090. doi: 10.1016/j.jcmg.2022.04.011. JACC Cardiovasc Imaging. 2022. PMID: 35680217 No abstract available.
References
-
- Ross R. Atherosclerosis — An Inflammatory Disease. New England Journal of Medicine 1999;340:115–126. - PubMed
-
- van der Wal AC, Becker AE, van der Loos CM, Das PK. Site of intimal rupture or erosion of thrombosed coronary atherosclerotic plaques is characterized by an inflammatory process irrespective of the dominant plaque morphology. Circulation 1994;89:36–44. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
