

External validation of the 4C Mortality Score for hospitalised patients with COVID-19 in the RECOVER network
- PMID: 35450898
- PMCID: PMC9023850
- DOI: 10.1136/bmjopen-2021-054700
External validation of the 4C Mortality Score for hospitalised patients with COVID-19 in the RECOVER network
Abstract
Objectives: Estimating mortality risk in hospitalised SARS-CoV-2+ patients may help with choosing level of care and discussions with patients. The Coronavirus Clinical Characterisation Consortium Mortality Score (4C Score) is a promising COVID-19 mortality risk model. We examined the association of risk factors with 30-day mortality in hospitalised, full-code SARS-CoV-2+ patients and investigated the discrimination and calibration of the 4C Score. This was a retrospective cohort study of SARS-CoV-2+ hospitalised patients within the RECOVER (REgistry of suspected COVID-19 in EmeRgency care) network.
Setting: 99 emergency departments (EDs) across the USA.
Participants: Patients ≥18 years old, positive for SARS-CoV-2 in the ED, and hospitalised.
Primary outcome: Death within 30 days of the index visit. We performed logistic regression analysis, reporting multivariable risk ratios (MVRRs) and calculated the area under the ROC curve (AUROC) and mean prediction error for the original 4C Score and after dropping the C reactive protein (CRP) component.
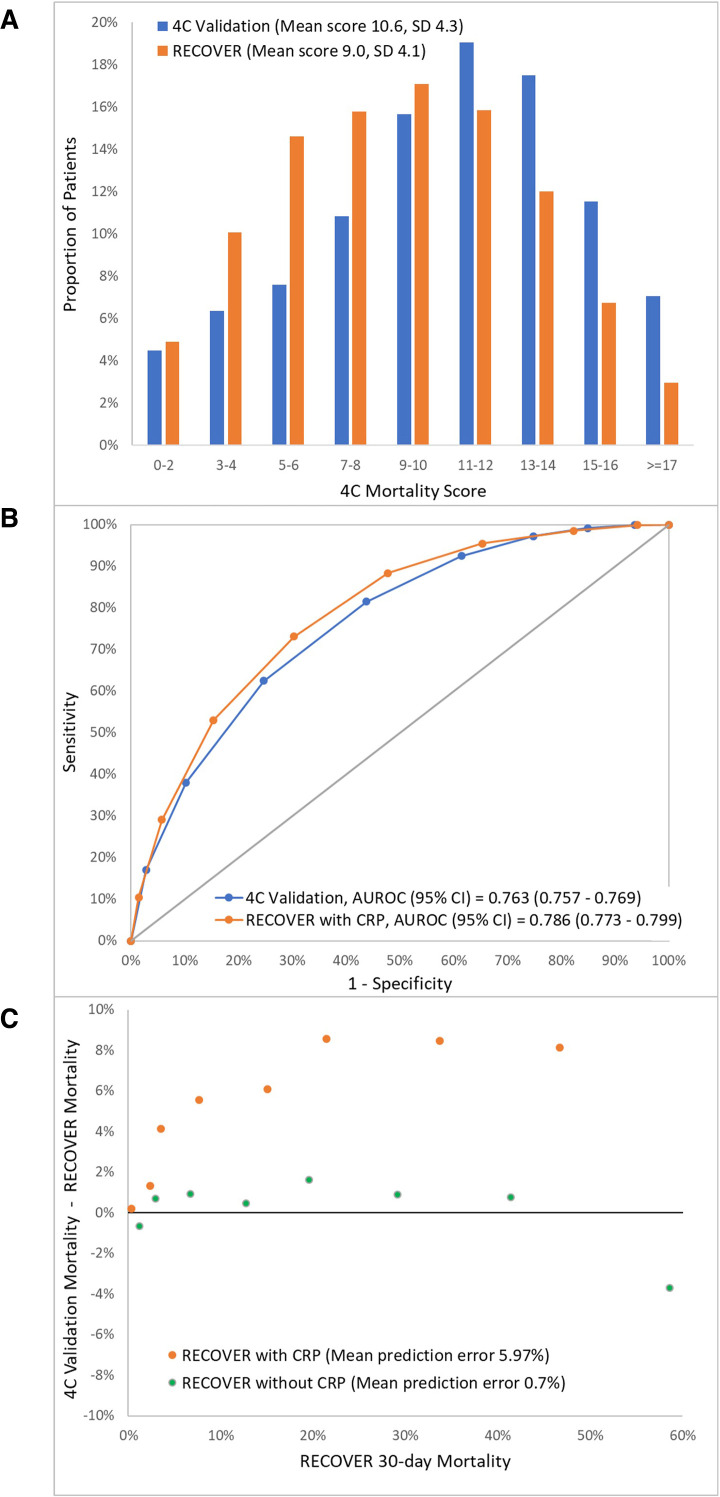
Results: Of 6802 hospitalised patients with COVID-19, 1149 (16.9%) died within 30 days. The 30-day mortality was increased with age 80+ years (MVRR=5.79, 95% CI 4.23 to 7.34); male sex (MVRR=1.17, 1.05 to 1.28); and nursing home/assisted living facility residence (MVRR=1.29, 1.1 to 1.48). The 4C Score had comparable discrimination in the RECOVER dataset compared with the original 4C validation dataset (AUROC: RECOVER 0.786 (95% CI 0.773 to 0.799), 4C validation 0.763 (95% CI 0.757 to 0.769). Score-specific mortalities in our sample were lower than in the 4C validation sample (mean prediction error 6.0%). Dropping the CRP component from the 4C Score did not substantially affect discrimination and 4C risk estimates were now close (mean prediction error 0.7%).
Conclusions: We independently validated 4C Score as predicting risk of 30-day mortality in hospitalised SARS-CoV-2+ patients. We recommend dropping the CRP component of the score and using our recalibrated mortality risk estimates.
Keywords: ACCIDENT & EMERGENCY MEDICINE; Adult intensive & critical care; COVID-19; EPIDEMIOLOGY; GENERAL MEDICINE (see Internal Medicine).
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
External validation of the 4C Mortality Score for patients with COVID-19 and pre-existing cardiovascular diseases/risk factors.BMJ Open. 2021 Sep 8;11(9):e052708. doi: 10.1136/bmjopen-2021-052708. BMJ Open. 2021. PMID: 34497086 Free PMC article. Clinical Trial.
-
Risk stratification of patients admitted to hospital with covid-19 using the ISARIC WHO Clinical Characterisation Protocol: development and validation of the 4C Mortality Score.BMJ. 2020 Sep 9;370:m3339. doi: 10.1136/bmj.m3339. BMJ. 2020. PMID: 32907855 Free PMC article.
-
Prospective validation of the 4C prognostic models for adults hospitalised with COVID-19 using the ISARIC WHO Clinical Characterisation Protocol.Thorax. 2022 Jun;77(6):606-615. doi: 10.1136/thoraxjnl-2021-217629. Epub 2021 Nov 22. Thorax. 2022. PMID: 34810237 Free PMC article.
-
External validation of six COVID-19 prognostic models for predicting mortality risk in older populations in a hospital, primary care, and nursing home setting.J Clin Epidemiol. 2024 Apr;168:111270. doi: 10.1016/j.jclinepi.2024.111270. Epub 2024 Feb 2. J Clin Epidemiol. 2024. PMID: 38311188
-
Rapid Evaluation of Coronavirus Illness Severity (RECOILS) in intensive care: Development and validation of a prognostic tool for in-hospital mortality.Acta Anaesthesiol Scand. 2022 Jan;66(1):65-75. doi: 10.1111/aas.13991. Epub 2021 Oct 15. Acta Anaesthesiol Scand. 2022. PMID: 34622441 Free PMC article.
Cited by
-
Discrimination of a single-item scale to measure intention to have a COVID-19 vaccine.PLoS One. 2025 May 5;20(5):e0322503. doi: 10.1371/journal.pone.0322503. eCollection 2025. PLoS One. 2025. PMID: 40323983 Free PMC article.
-
Prediction models based on machine learning algorithms for COVID-19 severity risk.BMC Public Health. 2025 May 13;25(1):1748. doi: 10.1186/s12889-025-22976-x. BMC Public Health. 2025. PMID: 40361078 Free PMC article.
-
Association between emergency department disposition and mortality in patients with COVID-19 acute respiratory distress syndrome.J Am Coll Emerg Physicians Open. 2024 Jun 16;5(3):e13192. doi: 10.1002/emp2.13192. eCollection 2024 Jun. J Am Coll Emerg Physicians Open. 2024. PMID: 38887225 Free PMC article.
-
Impact of Surge Strain and Pandemic Progression on Prognostication by an Established COVID-19-Specific Severity Score.Crit Care Explor. 2023 Dec 12;5(12):e1021. doi: 10.1097/CCE.0000000000001021. eCollection 2023 Dec. Crit Care Explor. 2023. PMID: 38094088 Free PMC article.
-
Serum transgelin is a novel prognostic biomarker for COVID-19 patients.Front Immunol. 2024 Nov 29;15:1423182. doi: 10.3389/fimmu.2024.1423182. eCollection 2024. Front Immunol. 2024. PMID: 39676863 Free PMC article.
References
-
- Ferrando C, Mellado-Artigas R, Gea A, et al. Patient characteristics, clinical course and factors associated to ICU mortality in critically ill patients infected with SARS-CoV-2 in Spain: a prospective, cohort, multicentre study. Rev Esp Anestesiol Reanim 2020;67:425–37. 10.1016/j.redar.2020.07.003 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous