

The Role of C-Reactive Protein as a Triage Tool for Pulmonary Tuberculosis in Children
- PMID: 35451001
- PMCID: PMC9302699
- DOI: 10.1093/jpids/piac015
The Role of C-Reactive Protein as a Triage Tool for Pulmonary Tuberculosis in Children
Abstract
Background: C-reactive protein (CRP) has shown promise as a triage tool for pulmonary tuberculosis (TB) in adults living with the human immunodeficiency virus. We performed the first assessment of CRP for TB triage in children.
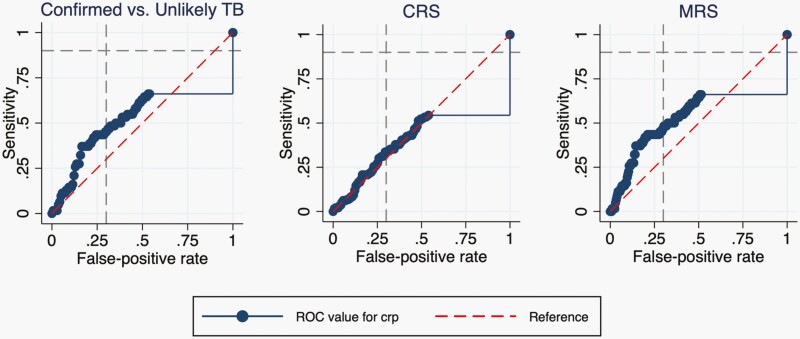
Methods: Symptomatic children less than 15 years old were prospectively enrolled in Kampala, Uganda. We completed a standard TB evaluation and measured CRP using a point-of-care assay. We determined the sensitivity and specificity of CRP to identify pulmonary TB in children using 10 mg/L and 5 mg/L cut-off points and generated a receiver operating characteristic (ROC) curve to determine alternative cut-offs that could approach the target accuracy for a triage test (≥90% sensitivity and ≥70% specificity).
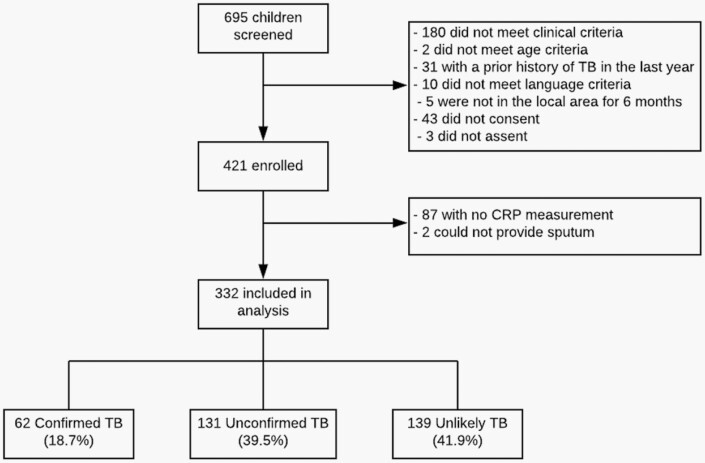
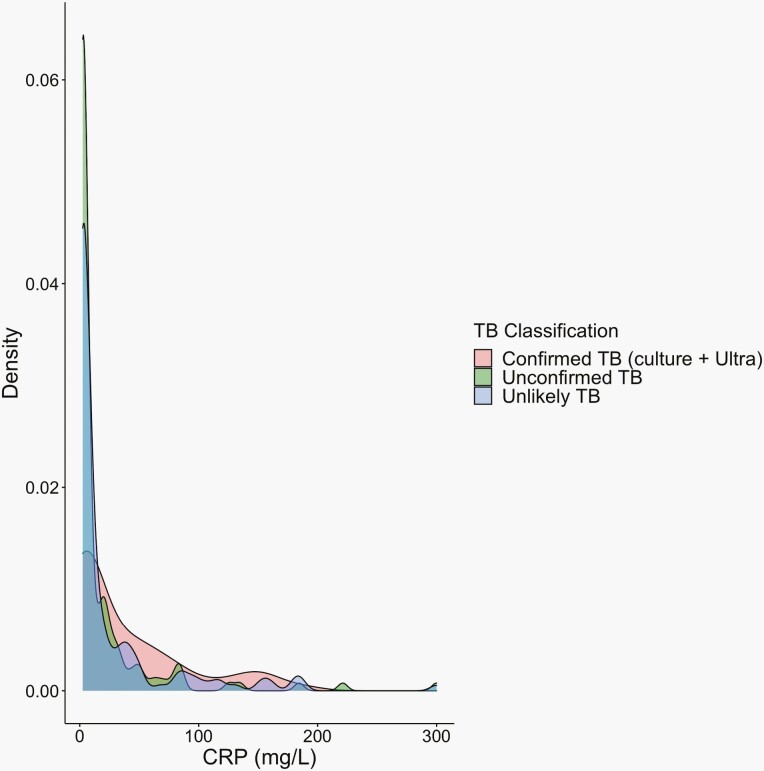
Results: We included 332 children (median age 3 years old, interquartile range [IQR]: 1-6). The median CRP level was low at 3.0 mg/L (IQR: 2.5-26.6) but was higher in children with Confirmed TB than in children with Unlikely TB (9.5 mg/L vs. 2.9 mg/L, P-value = .03). At a 10 mg/L cut-off, CRP sensitivity was 50.0% (95% confidence interval [CI], 37.0-63.0) among Confirmed TB cases and specificity was 63.3% (95% CI, 54.7-71.3) among children with Unlikely TB. Sensitivity increased to 56.5% (95% CI, 43.3-69.0) at the 5 mg/L cut-off, but specificity decreased to 54.0% (95% CI, 45.3-62.4). The area under the ROC curve was 0.59 (95% CI, 0.51-0.67), and the highest sensitivity achieved was 66.1% at a specificity of 46.8%.
Conclusions: CRP levels were low in children with pulmonary TB, and CRP was unable to achieve the accuracy targets for a TB triage test.
Keywords: C-reactive protein; child; triage; tuberculosis.
© The Author(s) 2022. Published by Oxford University Press on behalf of The Journal of the Pediatric Infectious Diseases Society. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Comment in
-
The Quest for a Child-Friendly Tuberculosis Triage Test.J Pediatric Infect Dis Soc. 2022 Jul 21;11(7):307-309. doi: 10.1093/jpids/piac020. J Pediatric Infect Dis Soc. 2022. PMID: 35451019 Free PMC article. No abstract available.
References
-
- World Health Organization. Roadmap Towards Ending TB in Children and Adolescents. Geneva: World Health Organization; 2018. Accessed January 18, 2020. https://www.who.int/tb/publications/2018/tb-childhoodroadmap/en/. Last.
-
- Marais BJ, Gie RP, Schaaf HS, et al. . The natural history of childhood intra-thoracic tuberculosis: a critical review of literature from the pre-chemotherapy era. Int J Tuberc Lung Dis 2004; 8:392–402. - PubMed
-
- Marais BJ, Gie RP, Schaaf HS, et al. . A proposed radiological classification of childhood intra-thoracic tuberculosis. Pediatr Radiol 2004; 34:886–94. - PubMed
-
- Starke JR, Donald PR.. Handbook of Child and Adolescent Tuberculosis. New York, NY: Oxford University Press; 2016.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
