

Efficacy of standardizing fibrinolytic therapy for parapneumonic effusion
- PMID: 35451632
- PMCID: PMC9023697
- DOI: 10.1007/s00247-022-05365-z
Efficacy of standardizing fibrinolytic therapy for parapneumonic effusion
Abstract
Background: While chest tube placement with pleural fibrinolytic medication is the established treatment of pediatric empyema, treatment failure is reported in up to 20% of these children.
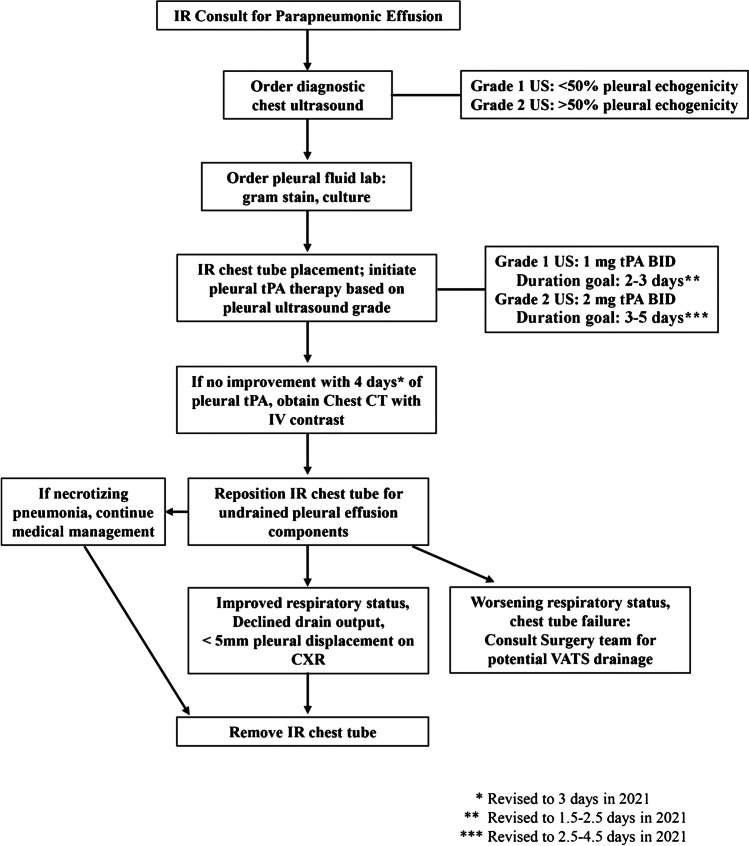
Objective: Standardizing fibrinolytic administration among interventional radiology (IR) physicians to improve patient outcomes in pediatric parapneumonic effusion.
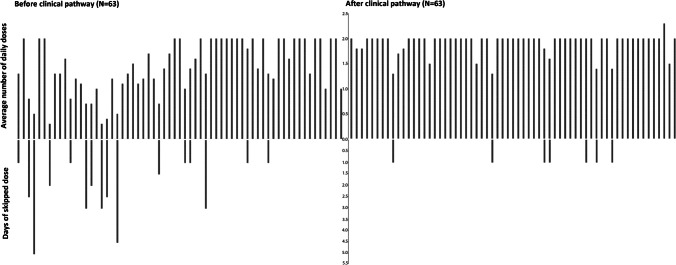
Materials and methods: We introduced a hospital-wide clinical pathway for parapneumonic effusion (1-2 mg tissue plasminogen activator [tPA] twice daily based on pleural US grade); we then collected prospective data for IR treatment May 2017 through February 2020. These data included demographics, co-morbidities, pediatric intensive care unit (PICU) admission, pleural US grade, culture results, daily tPA dose average, twice-daily dose days, skipped dose days, pleural therapy days, need for chest CT/a second IR procedure/surgical drainage, and length of stay. We compared the prospective data to historical controls with IR treatment from January 2013 to April 2017.
Results: Sixty-three children and young adults were treated after clinical pathway implementation. IR referrals increased (P = 0.02) and included higher co-morbidities (P = 0.005) and more PICU patients (P = 0.05). Mean doses per day increased from 1.5 to 1.9 (P < 0.001), twice-daily dose days increased from 38% to 79% (P < 0.001) and median pleural therapy days decreased from 3.5 days to 2.5 days (P = 0.001). No IR patients needed surgical intervention. No statistical differences were observed for gender/age/weight, US grade, need for a second IR procedure or length of stay. US grade correlated with greater positive cultures, need for chest CT/second IR procedure, and pleural therapy days.
Conclusion: Interventional radiology physician standardization improved on a clinical pathway for fibrinolysis of parapneumonic effusion. Despite higher patient complexity, pleural therapy duration decreased. There were no chest tube failures needing surgical drainage.
Keywords: Chest tube; Children; Clinical pathway; Empyema; Fibrinolytic; Interventional radiology; Parapneumonic effusion; Tissue plasminogen activator.
© 2022. The Author(s), under exclusive licence to Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
None
Figures
References
-
- Bradley JS, Byington CL, Shah SS, et al. Executive summary: the management of community-acquired pneumonia in infants and children older than 3 months of age: clinical practice guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America. Clin Infect Dis. 2011;53:617–630. doi: 10.1093/cid/cir625. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
