

Low rate of substantial loss of reduction immediately after hardware removal following acromioclavicular joint stabilization using a suspensory fixation system
- PMID: 35451639
- PMCID: PMC9568474
- DOI: 10.1007/s00167-022-06978-5
Low rate of substantial loss of reduction immediately after hardware removal following acromioclavicular joint stabilization using a suspensory fixation system
Abstract
Purpose: To evaluate immediate loss of reduction in patients undergoing hardware removal after arthroscopically assisted acromioclavicular (AC) joint stabilization using a high-tensile suture tape suspensory fixation system and to identify risk factors associated with immediate loss of reduction.
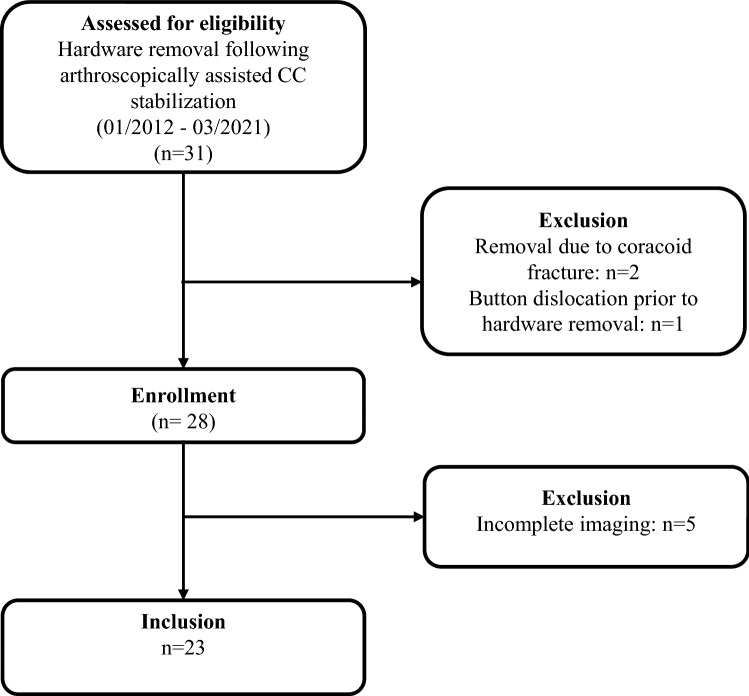
Materials and methods: Twenty-two consecutive patients with a mean age of 36.4 ± 12.6 years (19-56), who underwent hardware removal 18.2 ± 15.0 months following arthroscopically assisted stabilization surgery using a suspensory fixation system for AC joint injury between 01/2012 and 01/2021 were enrolled in this retrospective monocentric study. The coracoclavicular distance (CCD) as well as the clavicular dislocation/acromial thickness (D/A) ratio were measured on anterior-posterior radiographs prior to hardware removal and immediately postoperatively by two independent raters. Loss of reduction, defined as 10% increase in the CCD, was deemed substantial if the CCD increased 6 mm compared to preoperatively. Constitutional and surgical characteristics were assessed in a subgroup analysis to detect risk factors associated with loss of reduction.
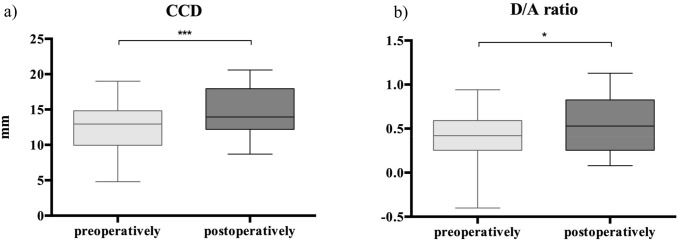
Results: Postoperatively, the CCD significantly increased from 12.6 ± 3.7 mm (4.8-19.0) to 14.5 ± 3.3 mm (8.7-20.6 mm) (p < 0.001) while the D/A ratio increased from 0.4 ± 0.3 (- 0.4-0.9) to 0.6 ± 0.3 (1.1-0.1) (p = 0.034) compared to preoperatively. In 10 cases (45%), loss of reduction was identified, while a substantial loss of reduction (> 6 mm) was only observed in one patient (4.5%). A shorter time interval between index stabilization surgery and hardware removal significantly corresponded to immediate loss of reduction (11.0 ± 5.6 vs. 30.0 ± 20.8 months; p = 0.007), as hardware removal within one year following index stabilization was significantly associated with immediate loss of reduction (p = 0.027; relative risk 3.4; odds ratio 11.67).
Conclusions: Substantial loss of reduction after hardware removal of a high-tensile suture tape suspensory fixation system was rare, indicating that the postoperative result of AC stabilization is not categorically at risk when performing this procedure. Even though radiological assessment of the patients showed a statistically significant immediate superior clavicular displacement after this rarely required procedure, with an increased incidence in the first year following stabilization, this may not negatively influence the results of ACJ stabilization in a clinically relevant way.
Level of evidence: IV.
Keywords: AC joint stabilization; Acromioclavicular joint injury; Acromioclavicular joint instability; Arthroscopically assisted; Hardware removal; Loss of reduction.
© 2022. The Author(s).
Conflict of interest statement
Authors Berthold DP., Muench LN, Rupp MC, Hinz M, Kadantsev P, Pogorzelski J, Scheiderer B and Feucht MJ declare that they have no conflict of interest. Siebenlist S is a consultant for Arthrex and Medi Bayreuth. Andreas B. Imhoff is a consultant for Arthrosurface and Medi Bayreuth and receives royalties from Arthrex and Arthrosurface.
Figures

References
-
- Beitzel K, Mazzocca AD, Bak K, Itoi E, Kibler WB, Mirzayan R, et al. ISAKOS upper extremity committee consensus statement on the need for diversification of the Rockwood classification for acromioclavicular joint injuries. Arthroscopy. 2014;30:271–278. doi: 10.1016/j.arthro.2013.11.005. - DOI - PubMed
-
- Berthold DP, Muench LN, Dyrna F, Uyeki CL, Cote MP, Imhoff AB, et al. Radiographic alterations in clavicular bone tunnel width following anatomic coracoclavicular ligament reconstruction (ACCR) for chronic acromioclavicular joint injuries. Knee Surg Sports Traumatol Arthrosc. 2021;29:2046–2054. doi: 10.1007/s00167-020-05980-z. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
