

MRI Allows Accurate Measurement of Glenoid Bone Loss
- PMID: 35452020
- PMCID: PMC9384911
- DOI: 10.1097/CORR.0000000000002215
MRI Allows Accurate Measurement of Glenoid Bone Loss
Abstract
Background: Bony Bankart lesions larger than a certain size can lead to a high redislocation rate, despite treatment with Bankart repair. Detection and measurement of glenoid bone loss play key roles in selecting the appropriate surgical therapy in patients with shoulder instability. There is controversy about which diagnostic modalities, using different measurement methods, provide the best diagnostic validity.
Questions/purposes: (1) What are the diagnostic accuracies of true AP radiographs, West Point (WP) view radiographs, MRI, and CT to detect glenoid bone loss? (2) Are there differences in the measurements of glenoid bone loss on MRI and CT? (3) What are the intrarater and interrater reliabilities of CT and MRI to measure glenoid bone loss?
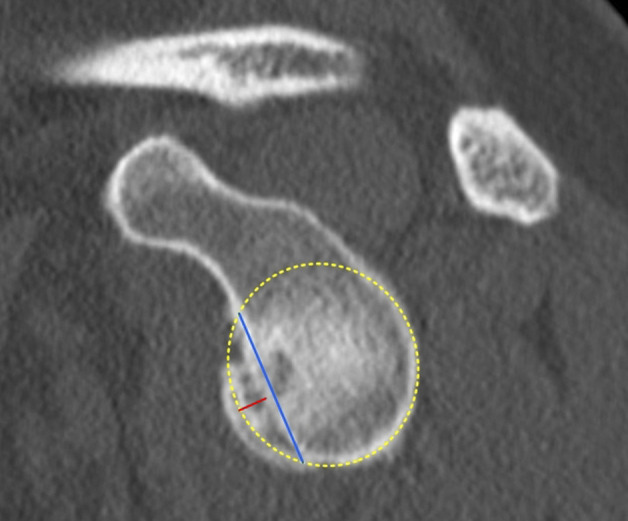
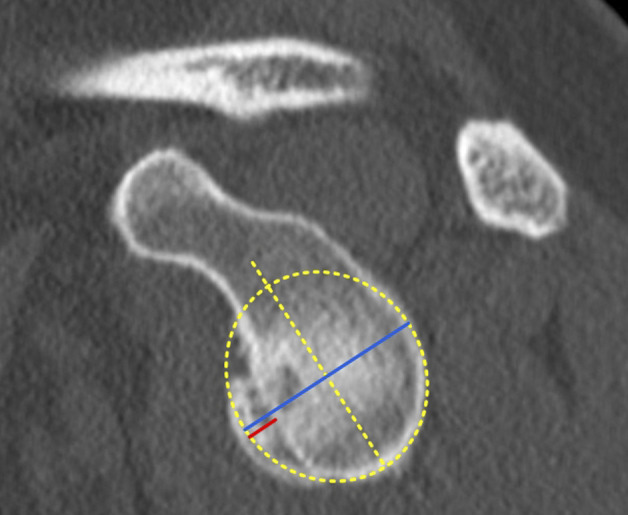
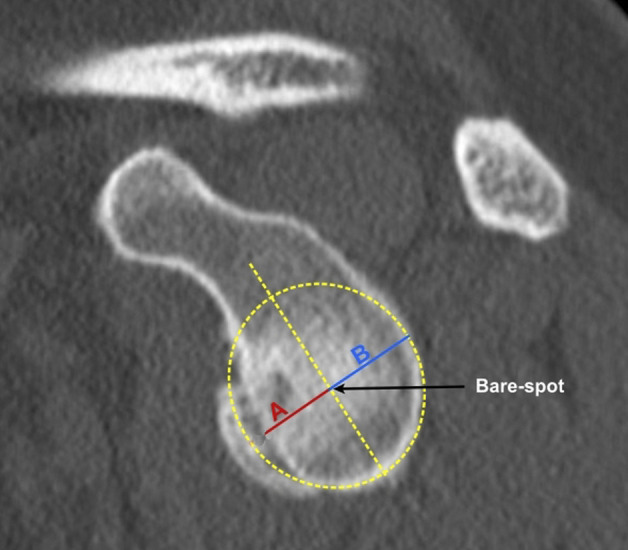
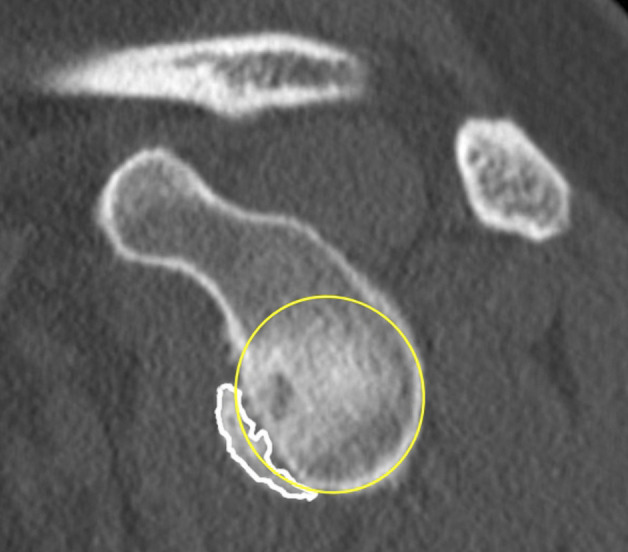
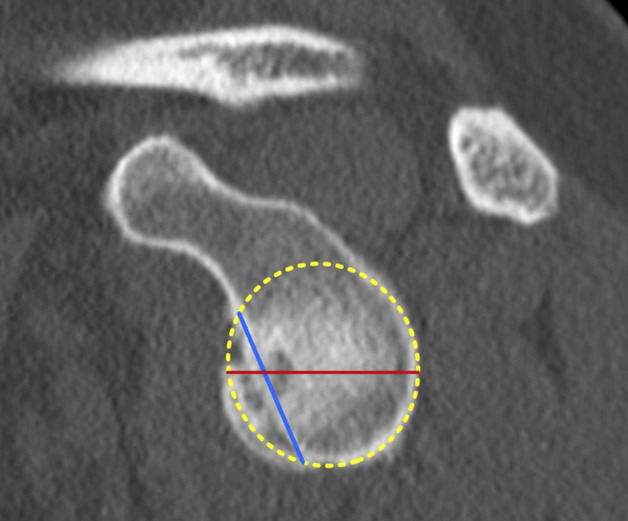
Methods: Between August 2012 and February 2017, we treated 80 patients for anterior shoulder instability. Of those, we considered patients with available preoperative true AP radiographs, WP radiographs, CT images, and MR images of the affected shoulder as potentially eligible. Based on that, 63% (50 of 80) of patients were eligible for analysis; 31% (25 of 80) were excluded because not all planes or slices (such as sagittal, axial, or frontal) of each diagnostic imaging modalities were available and 7% (5 of 80) because of the insufficient quality of diagnostic images (for example, setting of the layers did not allow adequate en face view of the glenoid). Preoperative true AP radiographs, WP radiographs, CT images and MR images of the affected shoulders were retrospectively assessed for the presence of glenoid bone loss by two blinded observers at a median (range) 25 months (12 to 66) postoperatively. To evaluate sensitivity, specificity, positive predictive value, negative predictive value, accuracy, diagnostic odds ratio, positive likelihood ratio, negative likelihood ratio, and area under the curve (AUC), we compared the detection of glenoid bone loss at follow-up achieved with the aforementioned imaging modalities with intraoperative arthroscopic detection. In all patients with glenoid bone loss, two blinded observers measured the size of the glenoid bone loss on preoperative CT and MR images using six measuring techniques: depth and length of the glenoid bone loss, Bigliani classification, best-fit circle width loss method, AP distance method, surface area method, and Gerber X ratio. Subsequently, the sizes of the glenoid bone loss determined using CT and MRI were compared. To estimate intraobserver and interobserver reliability, measurements were performed in a blinded fashion by two observers. Their level of experience was equivalent to that of orthopaedic residents, and they completed a training protocol before the measurements.
Results: For the ability to accurately diagnose Bankart lesions, the AUC (accuracy of a diagnostic test; the closer to 1.0, the more accurate the test) was good for MRI (0.83 [95% confidence interval 0.70 to 0.94]; p < 0.01), fair for CT (0.79 [95% CI 0.66 to 0.92]; p < 0.01), poor for WP radiographs (0.69 [95% CI 0.54 to 0.85]; p = 0.02) and failed for true AP radiographs (0.55 [95% CI 0.39 to 0.72]; p = 0.69). In paired comparisons, there were no differences between CT and MRI regarding (median [range]) lesion width (2.33 mm [0.35 to 4.53] versus 2.26 mm [0.90 to 3.47], p = 0.71) and depth (0.42 mm [0.80 to 1.39] versus 0.40 mm [0.06 to 1.17]; p = 0.54), and there were no differences concerning the other measurement methods: best-fit circle width loss method (15.02% [2.48% to 41.59%] versus 13.38% [2.00% to 36.34%]; p = 0.66), AP distances method (15.48% [1.44% to 42.01%] versus 12.88% [1.43% to 36.34%]; p = 0.63), surface area method (14.01% [0.87% to 38.25] versus 11.72% [2.45% to 37.97%]; p = 0.68), and Gerber X ratio (0.75 [0.13 to 1.47] versus 0.76 [0.27 to 1.13]; p = 0.41). Except for the moderate interrater reliability of the Bigliani classification using CT (intraclass correlation coefficient = 0.599 [95% CI 0.246 to 0.834]; p = 0.03) and acceptable interrater reliability of the Gerber X ratio using CT (0.775 [95% CI 0.542 to 0.899]; p < 0.01), all other measurement methods had good or excellent intrarater and interrater reliabilities on MRI and CT.
Conclusion: The results of this study show that CT and MRI can accurately detect glenoid bone loss, whereas WP radiographs can only recognize them poorly, and true AP radiographs do not provide any adequate diagnostic accuracy. In addition, when measuring glenoid bone loss, MRI images of the analyzed measurement methods yielded sizes that were no different from CT measurements. Finally, the use of MRI images to measure Bankart bone lesions gave good-to-excellent reliability in the present study, which was not inferior to CT findings. Considering the advantages including lower radiation exposure and the ability to assess the condition of the labrum using MRI, we believe MRI can help surgeons avoid ordering additional CT imaging in clinical practice for the diagnosis of anterior shoulder instability in patients with glenoid bone loss. Future studies should investigate the reproducibility of our results with a larger number of patients, using other measurement methods that include examination of the opposite side or with three-dimensional reconstructions.
Level of evidence: Level I diagnostic study.
Copyright © 2022 by the Association of Bone and Joint Surgeons.
Conflict of interest statement
Each author certifies that there are no funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article related to the author or any immediate family members. All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Figures
Similar articles
-
High Acromial Slope and Low Acromiohumeral Distance Increase the Risk of Retear of the Supraspinatus Tendon After Repair.Clin Orthop Relat Res. 2023 Jun 1;481(6):1158-1170. doi: 10.1097/CORR.0000000000002520. Epub 2022 Dec 20. Clin Orthop Relat Res. 2023. PMID: 36623210 Free PMC article.
-
Does Bone Loss Imaging Modality, Measurement Methodology, and Interobserver Reliability Alter Treatment in Glenohumeral Instability?Arthroscopy. 2020 Jan;36(1):12-19. doi: 10.1016/j.arthro.2019.06.025. Arthroscopy. 2020. PMID: 31864563
-
3-D CT is the most reliable imaging modality when quantifying glenoid bone loss.Clin Orthop Relat Res. 2013 Apr;471(4):1251-6. doi: 10.1007/s11999-012-2607-x. Epub 2012 Sep 21. Clin Orthop Relat Res. 2013. PMID: 22996361 Free PMC article.
-
Accuracy and reliability of imaging modalities for studying bipolar bone loss in anterior shoulder instability: A systematic review.Knee Surg Sports Traumatol Arthrosc. 2025 May;33(5):1844-1852. doi: 10.1002/ksa.12531. Epub 2024 Nov 4. Knee Surg Sports Traumatol Arthrosc. 2025. PMID: 39497437 Free PMC article.
-
Accuracy and Reliability of Imaging Modalities for the Diagnosis and Quantification of Hill-Sachs Lesions: A Systematic Review.Arthroscopy. 2021 Jan;37(1):391-401. doi: 10.1016/j.arthro.2020.08.005. Epub 2020 Aug 14. Arthroscopy. 2021. PMID: 32798670
Cited by
-
Association Between Rotator Cuff Tears and Shoulder MRI Parameters: Importance of Arthroscopic Validation in Coronal Acromiohumeral Interval Measurement.Orthop J Sports Med. 2025 Jan 21;13(1):23259671241309695. doi: 10.1177/23259671241309695. eCollection 2025 Jan. Orthop J Sports Med. 2025. PMID: 39845420 Free PMC article.
-
Comparison of reliability in two-dimensional computed tomography vs. two-dimensional magnetic resonance imaging for on-track/off-track measurements: analysis of key values for glenohumeral bone loss.JSES Int. 2025 Mar 17;9(4):1029-1033. doi: 10.1016/j.jseint.2025.02.014. eCollection 2025 Jul. JSES Int. 2025. PMID: 40703424 Free PMC article.
-
Current Concepts in the Measurement of Glenohumeral Bone Loss.Curr Rev Musculoskelet Med. 2023 Sep;16(9):419-431. doi: 10.1007/s12178-023-09852-0. Epub 2023 Jun 21. Curr Rev Musculoskelet Med. 2023. PMID: 37341857 Free PMC article. Review.
-
Inter-rater reliability in calculating glenoid bone loss among orthopedic surgeons and musculoskeletal radiologists: how much do we agree?JSES Int. 2025 Jan 14;9(3):603-606. doi: 10.1016/j.jseint.2024.12.010. eCollection 2025 May. JSES Int. 2025. PMID: 40486792 Free PMC article.
-
Bone loss in shoulder instability: putting it all together.Ann Jt. 2023 Jul 5;8:27. doi: 10.21037/aoj-23-6. eCollection 2023. Ann Jt. 2023. PMID: 38529222 Free PMC article. Review.
References
-
- Ali ZS, Hurley ET, Jamal MS, et al. Low rate of recurrent instability following the open Latarjet procedure as a revision procedure for failed prior stabilization surgery. Knee Surg Sports Traumatol Arthrosc. 2021;29:2110-2117. - PubMed
-
- Altan E, Ozbaydar MU, Tonbul M, Yalcin L. Comparison of two different measurement methods to determine glenoid bone defects: area or width? J Shoulder Elbow Surg. 2014;23:1215-1222. - PubMed
-
- Auffarth A, Mayer M, Kofler B, et al. The interobserver reliability in diagnosing osseous lesions after first-time anterior shoulder dislocation comparing plain radiographs with computed tomography scans. J Shoulder Elbow Surg. 2013;22:1507-1513. - PubMed
-
- Bakshi NK, Patel I, Jacobson JA, Debski RE, Sekiya JK. Comparison of 3-dimensional computed tomography-based measurement of glenoid bone loss with arthroscopic defect size estimation in patients with anterior shoulder instability. Arthroscopy. 2015;31:1880-1885. - PubMed
-
- LU Bigliani, Newton PM, Steinmann SP, Connor PM, McIlveen SJ. Glenoid rim lesions associated with recurrent anterior dislocation of the shoulder. Am J Sports Med. 1998;26:41-45. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
