

Clinical features of thrombosis and bleeding in COVID-19
- PMID: 35452509
- PMCID: PMC9040438
- DOI: 10.1182/blood.2021012247
Clinical features of thrombosis and bleeding in COVID-19
Abstract
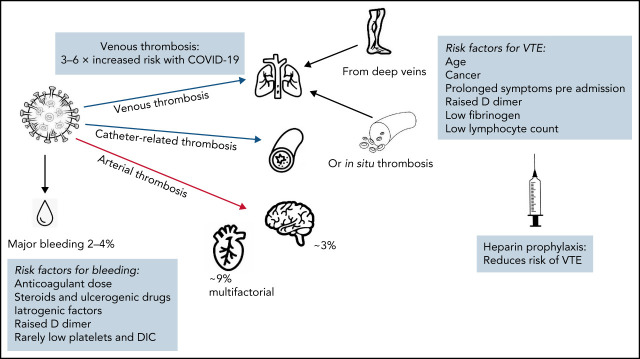
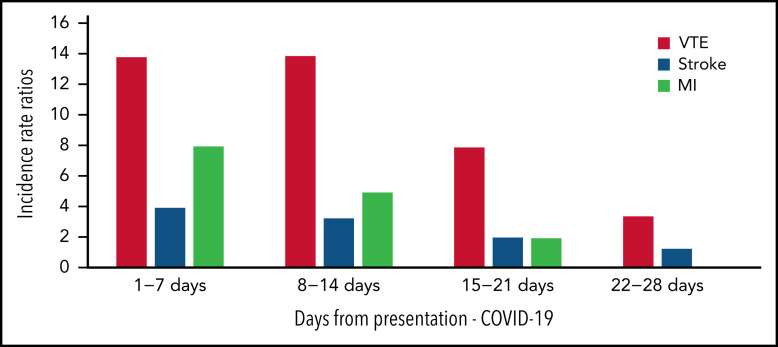
Infection with the SARS-CoV-2 virus, resulting in COVID-19 disease, has presented a unique scenario associated with high rates of thrombosis. The risk of venous thrombosis is some three- to sixfold higher than for patients admitted to a hospital for other indications, and for patients who have thrombosis, mortality appears to increase. Thrombosis may be a presenting feature of COVID-19. Pulmonary thrombi are the most frequent events, some related to deep vein thrombosis, but also to in situ microvascular and macrovascular thrombosis. Other venous thromboses include catheter- and circuit-associated in patients requiring hemofiltration and extracorporeal membrane oxygenation. Arterial thrombosis is less commonly documented, with 3% of patients in intensive care units having major arterial strokes and up to 9% having myocardial infarction, both of which are most likely multifactorial. Risk factors for thrombosis above those already documented in hospital settings include duration of COVID-19 symptoms before admission to the hospital. Laboratory parameters associated with higher risk of thrombosis include higher D-dimer, low fibrinogen, and low lymphocyte count, with higher factor VIII and von Willebrand factor levels indicative of more severe COVID-19 infection. All patients should receive thromboprophylaxis when admitted with COVID-19 infection, but the dose and length of treatment are still debated. Thrombosis continues to be treated according to standard VTE guidelines, but adjustments may be needed depending on other factors relevant to the patient's admission.
© 2022 by The American Society of Hematology.
Figures
References
-
- WHO Coronavirus (COVID-19) Dashboard . Geneva, Switzerland: World Health Organization; 2022. Available at: https://covid19.who.int. Accessed 1 October 2021.
-
- In: COVID-19 treatment Guidelines. Bethesda, MD: National Institutes of Health; 2022. Available at: https://www.covid19treatmentguidelines.nih.gov/overview/clinical-spectrum. Accessed 1 October 2021. - PubMed
-
- Helms J, Tacquard C, Severac F, et al. ; CRICS TRIGGERSEP Group (Clinical Research in Intensive Care and Sepsis Trial Group for Global Evaluation and Research in Sepsis) . High risk of thrombosis in patients with severe SARS-CoV-2 infection: a multicenter prospective cohort study. Intensive Care Med. 2020;46(6):1089-1098. - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
