

A Narrative Review on the Approach to Antimicrobial Use in Ventilated Patients with Multidrug Resistant Organisms in Respiratory Samples-To Treat or Not to Treat? That Is the Question
- PMID: 35453203
- PMCID: PMC9031060
- DOI: 10.3390/antibiotics11040452
A Narrative Review on the Approach to Antimicrobial Use in Ventilated Patients with Multidrug Resistant Organisms in Respiratory Samples-To Treat or Not to Treat? That Is the Question
Abstract
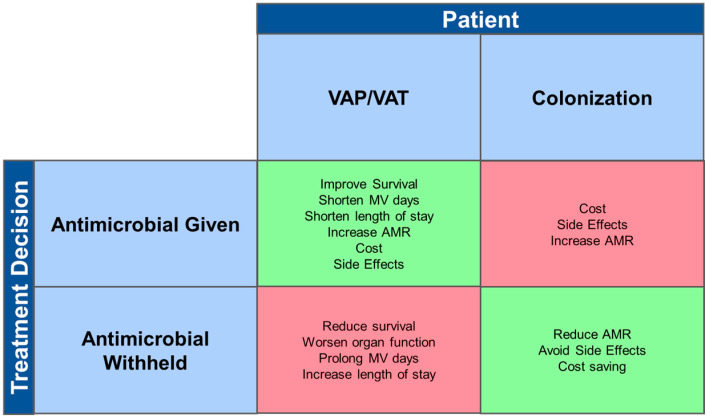
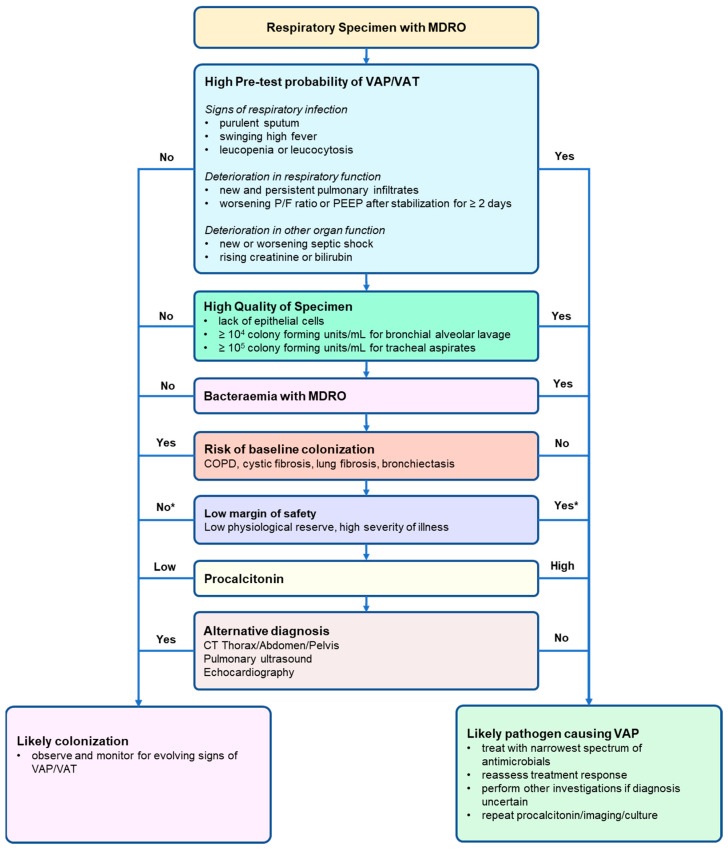
Multidrug resistant organisms (MDRO) are commonly isolated in respiratory specimens taken from mechanically ventilated patients. The purpose of this narrative review is to discuss the approach to antimicrobial prescription in ventilated patients who have grown a new MDRO isolate in their respiratory specimen. A MEDLINE and PubMed literature search using keywords "multidrug resistant organisms", "ventilator-associated pneumonia" and "decision making", "treatment" or "strategy" was used to identify 329 references as background for this review. Lack of universally accepted diagnostic criteria for ventilator-associated pneumonia, or ventilator-associated tracheobronchitis complicates treatment decisions. Consideration of the clinical context including signs of respiratory infection or deterioration in respiratory or other organ function is essential. The higher the quality of respiratory specimens or the presence of bacteremia would suggest the MDRO is a true pathogen, rather than colonization, and warrants antimicrobial therapy. A patient with higher severity of illness has lower safety margins and may require initiation of antimicrobial therapy until an alternative diagnosis is established. A structured approach to the decision to treat with antimicrobial therapy is proposed.
Keywords: ICU; decision; multidrug resistant; treatment; ventilator associated pneumonia; ventilator associated tracheobronchitis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Nseir S., Di Pompeo C., Pronnier P., Beague S., Onimus T., Saulnier F., Grandbastien B., Mathieu D., Delvallez-Roussel M., Durocher A. Nosocomial tracheobronchitis in mechanically ventilated patients: Incidence, aetiology and outcome. Eur. Respir. J. 2002;20:1483–1489. doi: 10.1183/09031936.02.00012902. - DOI - PubMed
-
- Luckraz H., Manga N., Senanayake E.L., Abdelaziz M., Gopal S., Charman S.C., Giri R., Oppong R., Andronis L. Cost of treating ventilator-associated pneumonia post cardiac surgery in the National Health Service: Results from a propensity-matched cohort study. J. Intensive Care Soc. 2018;19:94–100. doi: 10.1177/1751143717740804. - DOI - PMC - PubMed
-
- Melsen W.G., Rovers M.M., Groenwold R.H., Bergmans D.C., Camus C., Bauer T.T., Hanisch E.W., Klarin B., Koeman M., Krueger W.A., et al. Attributable mortality of ventilator-associated pneumonia: A meta-analysis of individual patient data from randomised prevention studies. Lancet Infect. Dis. 2013;13:665–671. doi: 10.1016/S1473-3099(13)70081-1. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
